
SMR Neurofeedback: The Calm-Alert Brainwave That Trains Sleep, Focus, and Self-Control
If you want one rhythm to anchor your understanding of neurofeedback, start with SMR, the sensorimotor rhythm.
SMR is a narrow band of low beta, roughly 12-15 Hz, generated over the sensorimotor strip, the ear-to-ear band of cortex that handles sensation and movement. It behaves like alpha for your motor system. The body goes quiet while the mind stays bright. You are still and ready at the same time.
It also sits at the origin of this field. SMR is the protocol that helped launch modern EEG biofeedback, and it remains one of the most reliable first-line training targets for sleep, anxiety stabilization, and impulse control.
What is SMR, and what is it doing in the brain?
People reach for "relaxation" to describe SMR, and that puts it in the wrong category. Relaxation usually means more alpha, the posterior dominant rhythm, plus a general drop in arousal. SMR is more specific than that. It is motor inhibition without cognitive shutdown. The body goes quiet while attention stays online.
SMR is also a particular strip rhythm, not a broad beta band, and you train it best over the sensorimotor cortex at C3, C4, or Cz.
The cleanest image I give people is the cat on the windowsill. Body perfectly still, attention locked on the world outside. That combination of quiet motor output and stable attention is SMR territory.
Why does SMR work? The gating mechanism
SMR rides on thalamocortical inhibition, and that mechanism is worth understanding because it explains everything else about this protocol.
The thalamus is your brain's switchboard. Almost everything you experience routes through thalamocortical loops, including sensory input, internal signals, and motor plans. When the switchboard leaks, signals get through that should have been filtered out. The consequences show up as sensory overwhelm, startle reactivity, restless movement, trouble staying asleep, and an attentional spotlight that won't hold still.
SMR training strengthens the inhibition and gating side of that loop. Less noise gets through, and the brain spends more of its time in a stable, regulated channel. This is well-established at the mechanistic level, and it is the reason SMR tends to help with several problems at once rather than one symptom in isolation. If you want the broader picture of how slowing and gating rhythms relate, the alpha waves explainer covers the idle-and-brakes side of the same system.
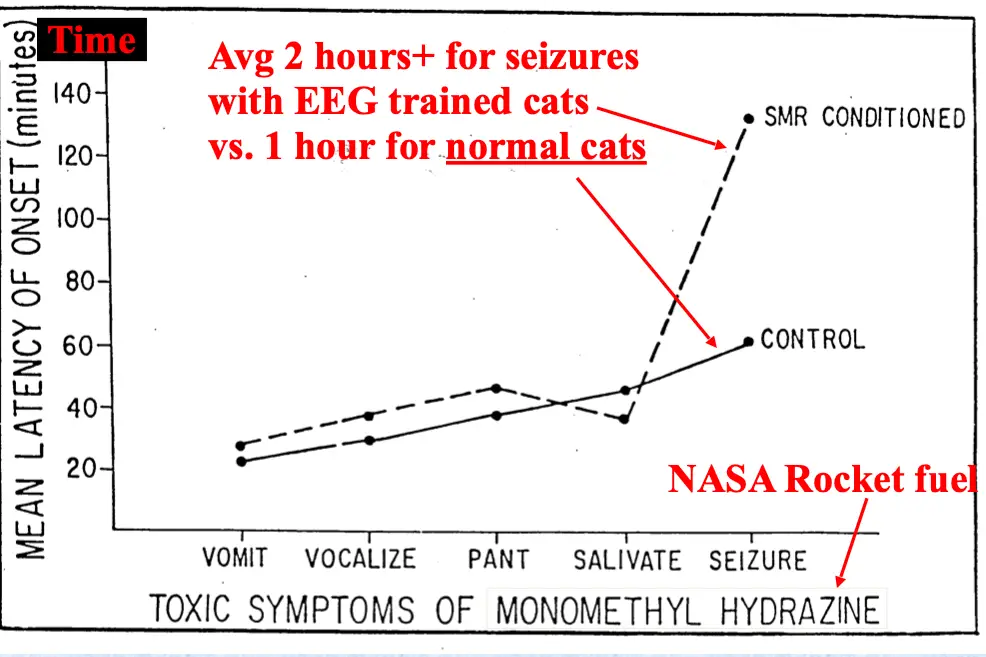
Where did SMR come from? Sterman's cats
SMR didn't earn its reputation from theory. It earned it from an accident in the lab.
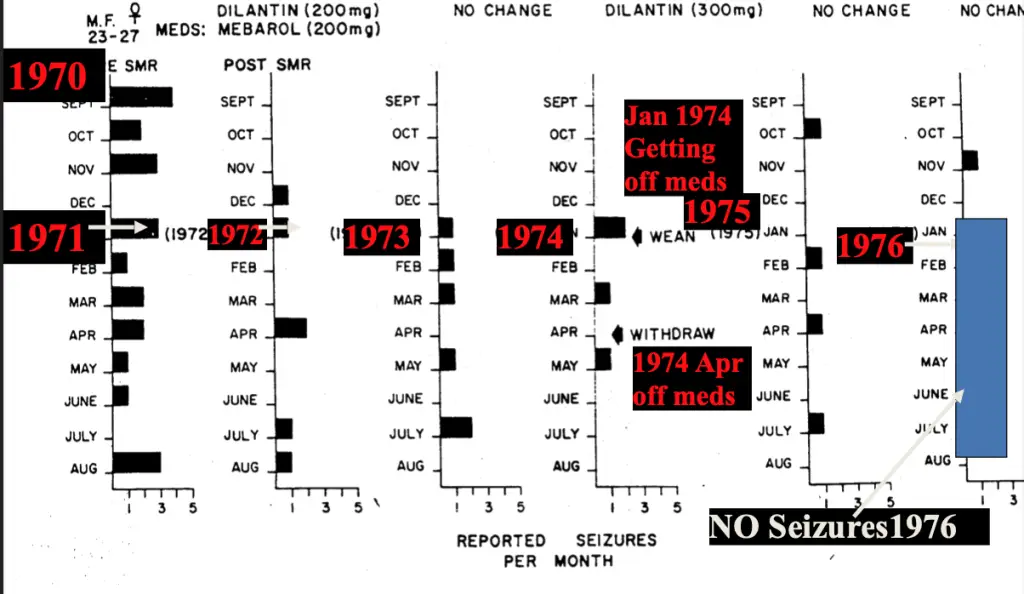
Barry Sterman at UCLA was studying the effects of rocket fuel exposure in cats. Some cats turned out to be unexpectedly seizure-resistant, and those cats had previously been trained to produce SMR-like activity. That observation opened decades of work on SMR as a stabilizing rhythm (Sterman & Fairchild, 1967; Sterman & Egner, 2006). For the full research base on neurofeedback for seizure and migraine, see the Peak Stability research collection.
Two reference figures from that line of work:
How does SMR help sleep?
SMR overlaps with sleep spindle physiology, the Stage 2 spindle bursts in particular. That overlap explains why SMR training is so often useful for the people who have the hardest time staying down.
Take too long to fall asleep, and you have long sleep onset latency. SMR training tends to shorten it. Feel tired but wired at bedtime, and you have hyperarousal insomnia, with the gating system stuck in scanning mode at the moment you need it to quiet. SMR works on that physiology directly. When sleep is shallow with frequent awakenings, strengthening spindle-band activity tends to deepen it.
There is a learning angle here too. Spindle dynamics relate to memory consolidation and skill acquisition. In one well-cited study, SMR training improved both sleep parameters and declarative learning outcomes (Hoedlmoser et al., 2008). For the wider sleep-architecture picture, see biohacking sleep.
What does SMR do for ADHD and impulsivity?
SMR sits right next to one of the classic ADHD findings. When the stability rhythm runs low, the brain leans into more disinhibited patterns.
In plain terms, low SMR makes it harder to inhibit movement and harder to hold attention steady, which is the popcorn-brain experience many people with ADHD describe. Training SMR up tends to improve impulse control and stabilize attention over a course of sessions.
SMR is not the only ADHD protocol, and I want to be honest that it is rarely used alone. It is a common starting point because it is stabilizing and it plays well with sleep, and sleep is often half the problem. ADHD is also not one thing in the EEG; the three confirmed brain patterns under one diagnosis shape which target makes sense. For the full picture of training in ADHD, read does neurofeedback work for ADHD.
What do results look like?
When SMR-focused training is matched to the person's EEG and run well, you tend to see a recognizable pattern over a course of sessions. The EEG shifts toward a more regulated baseline, with less noisy slow activity and more stable rhythms. Attention and response-control metrics improve on a CPT-style task.
Here is a representative before-and-after figure:
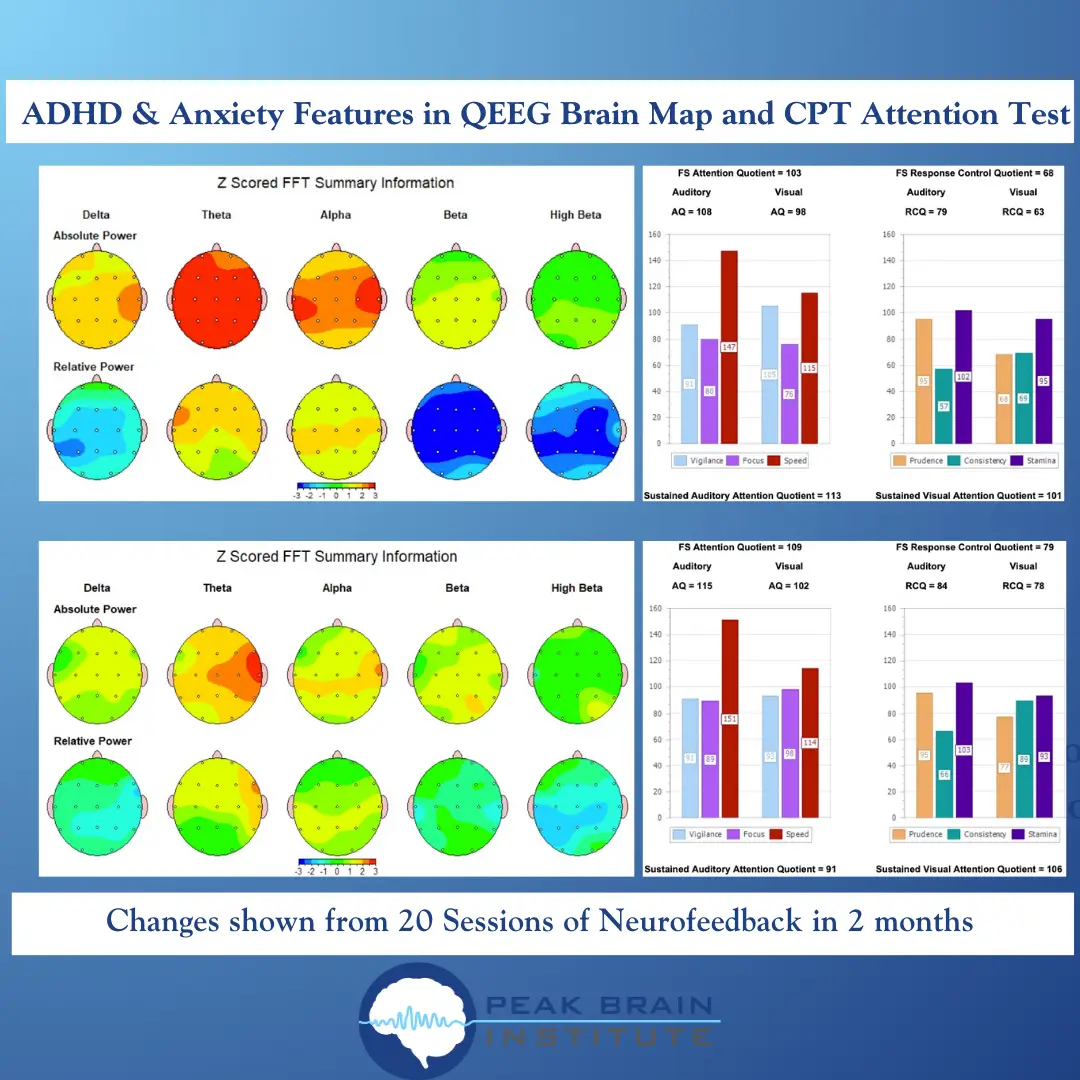
That figure shows roughly 20 sessions over about two months. The pattern is consistent with what I see in the maps, and individual response varies widely. The EEG you start with shapes the curve you get, and a meaningful share of people respond little or not at all. That is part of the territory and worth knowing before you start.
What happens in an SMR session?
SMR training is straightforward EEG biofeedback, and there is nothing mystical about the setup.
- Place an electrode at C3, C4, or Cz over the sensorimotor strip.
- Reference to an ear or mastoid and use a ground.
- Reward a narrow band around SMR, commonly 12-15 Hz, often individualized to your EEG.
- Inhibit slow activity (theta) and very fast activity (high beta) to cut artifacts and avoid tension training.
The after-effects tell you whether the setpoint is right. Train too fast for your system and you'll often feel wired later in the day, even if you felt calm during the session. Train too slow and you can get sleep disruption or a groggy, foggy feeling. Good neurofeedback is iterative for exactly this reason. You watch the after-effects and adjust the next session. A QEEG map gives you the starting target, and the QEEG brain mapping guide walks through what that assessment shows.
Who is SMR best for, and who should be cautious?
SMR is often a reasonable starting point for insomnia driven by hyperarousal physiology, for anxiety and panic stabilization, for ADHD and impulsivity features especially when sleep is also disrupted, and for post-concussion overstimulation patterns on a case-by-case basis.
Some presentations call for an experienced provider and clinical oversight rather than a self-directed setup. Seizure disorders need clinical supervision. Bipolar-spectrum instability makes protocol selection consequential. Severe trauma presentations should be stabilized first, with deeper protocols held back until the nervous system has a steadier baseline.
A word on choosing where to train, since SMR is so often a first protocol. A license or a board certification is at most a baseline-training signal. No research links specific neurofeedback credentials to better outcomes, and some of the most skilled practitioners built their skill over years of practice rather than a certification pathway. What actually predicts good work is whether the practitioner understands the technology and the neuroscience, individualizes from QEEG data instead of running a one-size-fits-all protocol, tracks outcomes with objective measures, re-maps every 20 to 25 sessions, and is honest about non-response. Be skeptical of high-pressure prepaid packages with no reassessment built in. Most neurofeedback is paid out of pocket, since many insurers classify it as investigational or not medically necessary, so this is real money that deserves real evaluation.
Where SMR fits
If neurofeedback had a foundation protocol, it would be SMR. The effect is not magic. It maps onto a real mechanism: better gating, better inhibition, more stable state control. Get that right and sleep gets easier, attention gets steadier, and the nervous system stops bracing as if a threat is always about to arrive.
If you want to start, get a QEEG map first so the SMR target is set to your physiology rather than a textbook average. For the broader evidence base, browse the neurofeedback training research library.
References (selected)
- Sterman, M. B., & Fairchild, M. D. (1967). SUBCONVULSIVE EFFECTS OF 1,1-DIMETHYLHYDRAZINE ON LOCOMOTOR PERFORMANCE ON THE CAT: RELATIONSHIP OF DOSE TO TIME OF ONSET. Defense Technical Information Center. https://doi.org/10.21236/AD0664549
- Sterman, M. B., & Egner, T. (2006). Foundation and practice of neurofeedback for the treatment of epilepsy. Applied Psychophysiology and Biofeedback, 31(1), 21-35. https://doi.org/10.1007/s10484-006-9002-x
- Hoedlmoser, K., Pecherstorfer, T., Gruber, G., Anderer, P., Doppelmayr, M., Klimesch, W., & Schabus, M. (2008). Instrumental conditioning of human sensorimotor rhythm (12-15 Hz) and its impact on sleep as well as declarative learning. Sleep, 31(10), 1401-1408.
TAGS
References
- Sterman (2006). Tracheobronchial stenting for management of bronchopleural fistula: a novel solution to an old problem. doi:10.1590/s0043-31442006000400014
- Sterman (1967). Subconvulsive effects of 1,1-dimethylhydrazine on locomotor performance in the cat. doi:10.21236/AD0664549
- Sterman (2006). Foundation and practice of neurofeedback for the treatment of epilepsy. doi:10.1007/s10484-006-9002-x
- Hoedlmoser (2008). Instrumental conditioning of human sensorimotor rhythm (12-15 Hz) and its impact on sleep as well as declarative learning. PMID 18853937
Get new articles and brain training insights by email.
No spam, unsubscribe anytime.
Related Articles
QEEG Brain Mapping: What It Is, What It Shows, and What to Expect
A neuroscientist explains what QEEG brain mapping measures, how it differs from a hospital EEG, what the maps show, and what happens during an assessment.
Does Neurofeedback Work for ADHD? A Neuroscientist's Guide
A clinical neuroscientist on what neurofeedback does for ADHD: the QEEG patterns, the evidence, session counts, and how to choose a real provider.
Why Does My ADHD Kid Make Me Yell? (And What to Do About It)
Your ADHD child's brain runs at low idle and needs high-intensity input to shift attention. Here's why yelling works, why it backfires, and what to do.
About Dr. Andrew Hill
Dr. Andrew Hill is a neuroscientist and pioneer in the field of brain optimization. With decades of experience in neurofeedback and cognitive enhancement, he bridges cutting-edge research with practical applications for peak performance.
Get Brain Coaching from Dr. Hill →