
Why Does My ADHD Kid Make Me Yell? (And What to Do About It)
You asked your child to put on their shoes fifteen minutes ago. They are still sitting on the floor, one shoe on, building a Lego tower, with no apparent awareness that you are late for school.
You ask again. Nicely. Nothing.
You ask louder. Still nothing.
Then you yell. Finally, movement. Your child jumps up, startled, and scrambles to get ready.
This happens daily. You hate it. You swore you would never be a yelling parent, and here you are.
Your child isn't ignoring you to be defiant. Their brain isn't generating enough activation signal to override the current focus, which is the Lego tower. A low-stimulus request like "please put on your shoes" doesn't cross the threshold needed to shift attention. A high-stimulus input like yelling does. ADHD brains respond to intensity because intensity is what they are tuned to detect.
You did not cause this, and your child didn't choose it. It is how attention dysregulation shows up in real life. Let me show you why ADHD brains need higher-intensity input, why yelling works in the moment while it damages everyone, and what you can do instead.
What Is Actually Happening in an ADHD Brain?
ADHD is a regulation problem, not an attention deficit. The brain can pay attention. It struggles to control where attention goes and when it shifts.
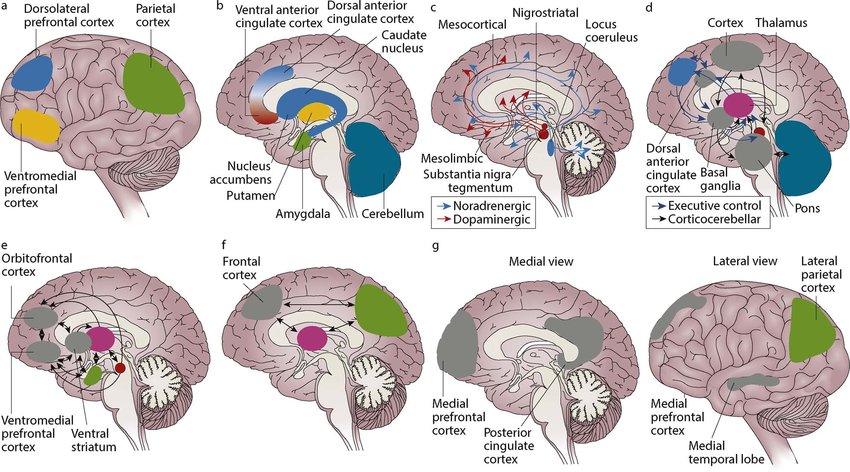
A few regions carry the load here, and each one explains a piece of the shoe-on-the-floor moment.
Prefrontal cortex (PFC). This is your executive control center: planning, task initiation, inhibition. In ADHD it tends to run hypoactive, especially the dorsolateral PFC. The result is difficulty starting tasks, weak impulse control, and attention that won't hold.
Anterior cingulate cortex (ACC). This region monitors conflict, catches errors, and helps select responses. In ADHD it often shows excess theta (4 to 8 Hz) where you would want more beta (13 to 30 Hz). The result is trouble arbitrating between competing demands, exactly the "play Lego" versus "put on shoes" conflict.
Right frontal regions. These handle motor inhibition, the brake that lets you stop yourself before acting. Reduced activation here shows up as impulsivity and difficulty with "wait" or "stop."
Sensorimotor cortex. This supports calm, focused attention and motor control. In ADHD you frequently see reduced SMR (sensorimotor rhythm, 12 to 15 Hz), which tracks with restlessness, trouble sitting still, and sleep problems.
On a QEEG, the signature pattern is elevated theta relative to beta in frontal regions. That ratio is the marker of cortical hypoarousal: the brain isn't generating enough "wake up" signal. This is well-established in the ADHD literature, and it is one of the most replicated EEG findings in the field. If you want the full picture of what a brain map shows and how it is read, I cover that in the QEEG brain mapping guide.
Here is the translation. Your child's brain is running at low idle. Low-intensity input doesn't generate enough signal to move attention. High-intensity input does. That is why your calm request bounces off and your yell lands.
Why Does Yelling Work in the Moment?

Yelling is poor parenting strategy and effective stimulation, and that combination is the trap. It works on the brain even when it fails the relationship.
A sudden loud sound activates the amygdala, your threat-detection system. That triggers a norepinephrine release, which raises alertness and sharpens attention. The brain shifts from low idle to high alert in a fraction of a second.
There is a dopamine component too. ADHD brains run with reduced dopamine availability or reduced receptor sensitivity, which is part of why low-reward tasks feel impossible to start. Intense stimulation drives a dopamine release, and that creates a perverse lesson: escalation brings clarity.
Yelling also breaks the current hyperfocus. The core problem in ADHD is shifting attention, not holding it. Once the brain locks onto something engaging, a Lego build or a video game or a daydream, moving off it requires a strong signal. Yelling is a strong signal.
Then the feedback loop forms. You ask calmly, a low stimulus, and nothing registers. You escalate to a moderate stimulus, and still nothing. You yell, a high stimulus, and finally there is enough arousal to shift attention, so your child moves. Run that cycle a few hundred times and the brain learns to tune out low-intensity requests entirely. Only yelling, urgency, or punishment produces a response. You have unintentionally trained a threshold problem.
Why Does Yelling Hurt Both of You?

For the child, repeated yelling means chronic activation of the threat response, shame loops ("I'm bad," "I can't do anything right"), and a slide toward learned helplessness where they only move under external pressure and never build internal regulation. It also reshapes the relationship, so you become a source of stress instead of a source of safety.
For you, the cost is guilt, exhaustion from constant escalation, and resentment that builds when "why can't they just listen" becomes the soundtrack of every morning. You end up cast as the enforcer rather than the nurturer, and that role wears on both of you.
How Do I Provide Intensity Without Yelling?

Your child needs higher-intensity input to shift attention. The skill is delivering that intensity without triggering a threat response. Each of these gives the brain a strong signal through a channel other than fear.
Use Visual Cues Instead of Volume
Hold up a brightly colored object while you speak. Use a flashlight, shining it on your child and then on the task. Write the request on a whiteboard instead of saying it. Use a hand signal or gesture.
Visual novelty triggers the orienting response, an automatic attention shift, without firing the amygdala the way yelling does. You get the attention grab without the stress hit.
Get Close and Add Touch
Walk over to your child, put a hand on their shoulder, make eye contact, and then speak. Kneel to their level, which lowers the power differential and feels less threatening. Use gentle touch to break the current focus before you give the instruction.
Proximity and touch raise arousal without activating the threat circuit. Your child registers your physical presence more strongly than your words from across the room.
Cut the Words, Keep the Clarity
Working memory in ADHD typically holds fewer items, often in the range of three to five, so multi-step instructions overflow capacity before they can be executed. Long explanations don't land.
Give one instruction at a time, five words or fewer. Instead of "It's time to get ready for school so please go put on your shoes and get your backpack and don't forget your lunch," say "Shoes. Now," and point to the shoes. Once the shoes are on: "Backpack. Now," and point. A single instruction stays in working memory long enough to act on.
Let a Timer Be the Pressure
Use a timer, ideally one with both a visual countdown and a sound, to create urgency without you escalating. "You have five minutes to finish this. Timer starts now." "When the timer beeps, Legos go away and shoes go on." A Time Timer, kitchen timer, or phone alarm all work.
The timer becomes the source of urgency instead of you. Your child responds to the beep and the shrinking countdown, and the conflict moves off the parent-child relationship.
Build in Movement
ADHD brains regulate through movement. Forcing stillness increases restlessness and lowers compliance, so embed motion into the routine. "Put on one shoe, do ten jumping jacks, put on the other shoe." "After homework page one, run around the house once." Let homework happen standing, pacing, or on an exercise ball.
Movement raises arousal, dopamine, and norepinephrine, which brings the brain up to the activation level it needs to execute the task. You are using physiology instead of fear to lift the idle.
Warn Before You Transition
Shifting from one activity to the next is one of the hardest moments for an ADHD brain. Give a heads-up before the demand lands. "In five minutes we're leaving. Start wrapping up." "Two more minutes of screen time, then bedtime." Pair it with a visual countdown when you can.
The warning gives the brain time to prepare for the shift. An immediate transition feels jarring and pulls resistance up by reflex.
What Are the Long-Term Fixes?

The strategies above manage the moment. These raise your child's baseline regulation so the moments get easier.
Fix the Sleep First
Sleep problems are endemic in ADHD, and poor sleep worsens every symptom: attention, impulsivity, emotional control. Reduced SMR (12 to 15 Hz) makes it hard to quiet the motor system at night. The circadian rhythm often runs phase-delayed, producing genuine night owls. And the day's stimulation lingers as racing thoughts at bedtime.
Lock a consistent wake time, including weekends, which matters more than the bedtime. Get morning light exposure, 30 to 60 minutes outdoors. Build an evening routine with dimmed lights and enough physical activity to burn off restlessness. Neurofeedback in the range of 20 to 40 sessions can improve sleep and impulse control. Better sleep improves prefrontal function, which improves self-regulation, which lowers the demand for your escalation.
Train the Theta-Beta Ratio with Neurofeedback
If your child has been QEEG-mapped and shows an elevated theta-beta ratio, neurofeedback targets exactly that pattern. The protocol trains down theta (4 to 8 Hz) at frontal sites and rewards beta (13 to 20 Hz) or SMR (12 to 15 Hz), usually across 30 to 40 sessions over three to four months.
Multiple studies show neurofeedback reducing ADHD symptoms comparably to stimulant medication, with effects that persist 6 to 12 months after training ends. The expected outcome is higher baseline arousal, less of that "brain fog" feeling, better sustained attention, and improved impulse control. For a fuller account of the evidence base and what to expect, see my neurofeedback for ADHD guide.
Consider Medication When It Fits
Stimulant medication, methylphenidate or amphetamines, increases dopamine and norepinephrine and improves prefrontal function. The practical effect is a higher baseline arousal, so your child can respond to a normal-intensity request without you having to yell.
Work with the prescribing physician. Watch sleep, since stimulants taken too late in the day worsen it. Track effectiveness with a rating scale like the Vanderbilt. Medication helps, and it does not replace behavioral strategy, sleep, and structure.
Build External Structure
ADHD brains lean on external structure to make up for weak internal regulation. Use visual schedules, a morning routine chart and an after-school chart. Keep timing consistent, with wake, meals, homework, and bed landing at the same times each day. Make consequences predictable, so if X happens, Y follows, every time.
External structure stands in for the executive function that is running weak. Over time the routines harden into habits encoded in the basal ganglia, which need far less prefrontal effort to run.
What About Your Own Brain?
You cannot regulate your child while you are dysregulated, and ADHD parenting attacks your regulation directly.
Sleep deprivation weakens your own prefrontal cortex. Chronic stress shifts you toward automatic, reactive patterns. Decision fatigue sets in, so by five in the evening your executive function is depleted and the yell is already loaded.
So prioritize your own sleep, seven to nine hours, non-negotiable, because your prefrontal cortex needs it to stay regulated. Run a daily stress practice, ten to twenty minutes of meditation or breathwork, and add HRV training to build stress resilience. Find social support from other ADHD parents who actually get it.
Lower the expectations that keep ammunition in the chamber. Your ADHD child will not perform like neurotypical peers, progress is measured in months and years rather than days, and small wins are worth marking.
When you do lose it, repair. "I'm sorry I yelled. That wasn't okay." Say what you will try differently next time. Repairing after a rupture models self-regulation and teaches your child the emotional skill directly, which is worth more than never rupturing at all.
Where to Start Tomorrow Morning
Your child isn't ignoring you. Their brain needs higher-intensity input to shift attention, and yelling supplies that intensity at the cost of stress, shame, and a damaged relationship.
Tomorrow, pick two of the in-the-moment tools and use them before you raise your voice. Walk over, put a hand on the shoulder, make eye contact, and say "Shoes. Now." Set a timer for the morning routine and let it carry the urgency. Cut your instructions to five words.
Then start the longer work: lock a consistent wake time for both of you, get morning light, and if you have access to a QEEG, find out whether your child's theta-beta ratio is elevated so you know whether neurofeedback fits.
You are providing external regulation for a brain that can't yet regulate itself, and that is genuinely exhausting. Work with the difference, intensity without threat and structure without rigidity, and both of you carry less of the load. One interaction at a time.
Get new articles and brain training insights by email.
No spam, unsubscribe anytime.
Related Articles
SMR Neurofeedback: The Calm-Alert Brainwave That Trains Sleep, Focus, and Self-Control
SMR is the 12-15 Hz sensorimotor rhythm that trains sleep, focus, and impulse control. A neuroscientist explains the gating mechanism and the evidence.
Procrastination: Biohacking Your Brain for Action
Procrastination is a neural cost-benefit loop, not a character flaw. Learn the circuits behind avoidance and the biohacking strategies that retrain them.
ADHD Brain Types: Three Confirmed Patterns, One Diagnosis
Three confirmed ADHD brain types, the sleep and hyperarousal that ride along, and why matching treatment to your brain matters more than the DSM label.
About Dr. Andrew Hill
Dr. Andrew Hill is a neuroscientist and pioneer in the field of brain optimization. With decades of experience in neurofeedback and cognitive enhancement, he bridges cutting-edge research with practical applications for peak performance.
Get Brain Coaching from Dr. Hill →