The Critical Aging Window: Why Your Brain Starts Aging at 44, Not 70
If you are 44 or older, your brain networks are already destabilizing. The driver is metabolic stress, specifically your neurons' declining ability to import glucose for fuel.
This is well-established. Mujica-Parodi and colleagues (2020, PNAS) analyzed functional connectivity in over 19,300 people and found a sharp transition at age 44. Before that point, brain networks are remarkably stable. After 44, they begin to fragment. By 67, the deterioration accelerates.
The mechanism is neuronal insulin resistance: your brain cells losing the ability to bring glucose across the membrane even when blood sugar is normal. Some researchers call it "type 3 diabetes," brain-specific. You can have it while your body's metabolism looks perfect on a standard panel.
The metabolic dysfunction begins decades before any cognitive symptom appears. By the time someone struggles with memory in their 70s, their neurons have been energy-starved since their 40s. The same study points to an intervention window, roughly ages 40 to 59, when metabolic support can stabilize the networks. After 60 the window starts closing, because vascular damage and neuronal death become irreversible.
Is brain aging gradual, or does it happen in jumps?
For decades the assumption was that brain aging is linear, a slow steady decline from age 20 onward. The data say otherwise.
The Stony Brook study measured functional connectivity across more than 19,300 individuals and found an S-shaped curve with three distinct transitions.
Transition 1: Age 44, the bend before the break
Brain networks begin destabilizing. Connections between regions weaken and metabolic stress becomes measurable on fMRI. Cognitive function still looks normal because compensation is working.
You do not notice because your brain is good at compensating. It recruits additional regions, shifts metabolic processes, and upregulates backup systems. Tests of memory and attention come back fine. Underneath, your neurons are running on diminishing energy. Picture a business operating on shrinking cash reserves: operations look normal from the outside while the balance sheet erodes.
Transition 2: Age 60 to 67, rapid acceleration
Network deterioration speeds up. Vascular effects compound, including small vessel disease and white matter lesions. Compensation starts failing and cognitive symptoms surface: memory lapses, slower processing, word-finding trouble.
The decline feels sudden, but it has been building for 15 to 20 years. What accelerates is the failure of compensation. Once the system can no longer keep up, the loss becomes obvious. A dam with a slow leak holds for years while you patch it, then the patches give out together.
Transition 3: Age 90 and beyond, plateau
Deterioration slows, likely because the most vulnerable neurons have already died and the survivors are more resilient. This plateau reflects the exhaustion of vulnerable cells, not recovery.
Why can't an aging brain use glucose normally?
Your brain's energy demand is enormous
Your brain is 2% of body weight and consumes about 20% of your body's energy. It burns roughly 120g of glucose per day, the equivalent of 480 calories. Glucose cannot diffuse into neurons on its own; it needs a transporter.
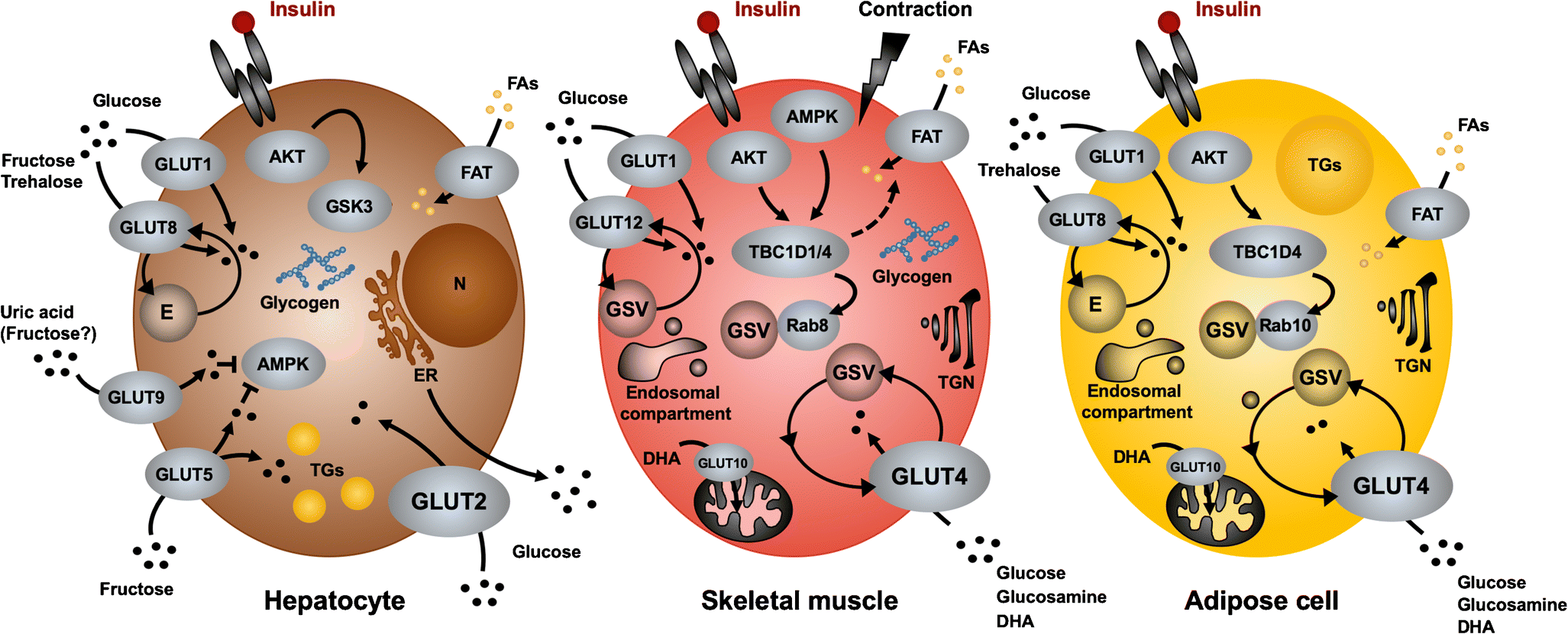
The GLUT4 system, and where it breaks
In normal glucose metabolism, glucose sits in the bloodstream, insulin signals the neuron that fuel is available, the neuron moves GLUT4 transporters to its membrane, and glucose enters to run through glycolysis, the Krebs cycle, and ATP production.
In neuronal insulin resistance, glucose is present, insulin is present and sometimes elevated, but the GLUT4 response is blunted. Glucose cannot get in. The neuron starves while surrounded by fuel.
This is distinct from type 2 diabetes. You can have normal blood sugar, no metabolic syndrome, and a healthy weight, and still develop neuronal insulin resistance. The brain's insulin signaling runs semi-independently from the body's.
Why does the shift land near age 44?
Several mechanisms are proposed. Decades of reactive oxygen species damage insulin receptors. Low-grade systemic inflammation impairs insulin signaling. Aging mitochondria produce less ATP, which feeds back into the problem. Years of a high-carb diet may desensitize receptors.
The data give the sequence. Metabolic changes precede vascular changes; they are not parallel. Brain glucose hypometabolism is detectable 10 to 20 years before an Alzheimer's diagnosis (Cunnane et al., 2016). APOE ε4 carriers show worse insulin-resistance effects. Neuronal insulin resistance sits upstream of the pathology. Amyloid plaques, tau tangles, and vascular damage are downstream consequences. That is a well-supported inference from the imaging timeline, though the causal chain is still being worked out.
The compensation phase, ages 44 to 60
You do not feel decline in your 40s and 50s because the brain compensates. It recruits additional regions to finish a task, switching from unilateral to bilateral activation. It shifts metabolic pathways, leaning more on lactate and astrocyte support. It strengthens synapses to make up for fewer functional neurons.
Compensation is metabolically expensive. It holds for a while, then runs out. By your 60s the compensation machinery itself starts to fail. Normal cognitive tests in your 50s mean your brain is compensating well for now. The underlying stress is real.
Can ketones feed a brain that can't use glucose?
When researchers identified neuronal insulin resistance, the solution was already in your metabolic toolkit: ketones.
How ketones get in without insulin
You produce ketones, beta-hydroxybutyrate and acetoacetate, when you fast for 12 or more hours, follow a ketogenic diet under 50g of carbs per day, take exogenous ketone supplements, or exercise intensely enough to reach mild ketosis.
The critical difference is the door they use. Glucose depends on GLUT4, which depends on insulin. Ketones cross through MCT2 transporters, which do not require insulin. MCT2 is the express lane that bypasses the traffic jam. Once inside, ketones feed acetyl-CoA into the Krebs cycle and produce ATP as effectively as glucose would.
The intervention study
Mujica-Parodi's team tested this directly. They gave 101 participants ketone drinks and measured brain network stability on fMRI. Ketones significantly stabilized the networks. The effect was strongest in ages 40 to 59, the critical window. Glucose supplementation did nothing, which fits the mechanism: the problem is insulin resistance, not glucose availability.
| Age Group | Brain State | Ketone Response |
|---|---|---|
| 20-39 | Stable, pre-destabilization | Minimal benefit (networks already stable) |
| 40-59 | Metabolic stress, still viable neurons | Maximum benefit, critical window |
| 60-79 | Vascular damage, some neuronal death | Diminished benefit (too late for many neurons) |
| 90+ | Severe decline | Not studied, likely minimal effect |
Ketones rescue metabolically stressed neurons. They cannot resurrect dead ones. You intervene while neurons are struggling but viable.
Why does timing matter so much in the 40-59 window?
This is the core finding. Metabolic interventions work best before symptoms appear, during the bend before the break.
In your 40s and 50s, neurons are metabolically stressed but still alive and functional, compensation is working, and intervention can stabilize them. In your 60s and 70s, years of energy starvation have triggered cascades: endothelial dysfunction and small vessel disease, impaired amyloid clearance, microglial neuroinflammation, and neuronal apoptosis. Much of that is irreversible, and intervention loses traction.
This is also why most Alzheimer's drug trials fail. They enroll people in their 60s and 70s who already have symptoms, trying to rescue neurons that died 15 to 20 years earlier. The strategic implication is straightforward: start metabolic support in your 40s, while neurons are stressed but salvageable.
What can you do during the critical window?

Here is what the science supports if you are in the 40 to 59 range.
Tool 1: Periodic ketosis
The goal is regular ketone access without permanent dietary restriction.
- Intermittent fasting (16:8): fast 16 hours, eat in an 8-hour window. Mild ketosis kicks in after 12 to 14 hours. Start here, 5 days a week. For the full breakdown, see Strategic Fasting.
- Weekly 24 to 36 hour fast: once a week, skip dinner through the next day's lunch for deeper ketosis.
- Periodic ketogenic diet: 1 to 2 weeks per quarter under 50g of carbs per day.
- Exogenous ketones: ketone esters or salts on non-fasting days, rapid ketosis in 30 to 60 minutes.
Tool 2: Exercise, the insulin sensitizer
Exercise improves neuronal insulin sensitivity through several routes. It activates AMPK, a metabolic sensor that upregulates glucose transporters. It lowers inflammation that interferes with insulin signaling. It raises BDNF, which supports neuronal health and metabolic function. Prolonged aerobic work also pushes you into mild ketosis.
A workable protocol: 30 to 60 minutes of Zone 2 aerobic work at a conversational pace, 4 to 5 times a week; strength training 2 to 3 times a week to preserve muscle mass and metabolic health; HIIT 1 to 2 times a week for maximal AMPK activation. Aerobic exercise improves glucose metabolism in aging brains (Erickson et al., 2011), and it is probably the single most effective intervention for neuronal insulin sensitivity.
Tool 3: Sleep
Sleep deprivation impairs glucose metabolism throughout the body, brain included. One night of poor sleep drops insulin sensitivity by 20 to 30%. Keep a consistent wake time seven days a week, get 7 to 9 hours total, and protect deep sleep in the first 3 to 4 hours of the night. Track it with an Oura Ring, Whoop, or a simple sleep diary. For the mechanisms, see Biohacking Sleep.
Tool 4: Anti-inflammatory diet
Chronic inflammation impairs insulin signaling, so lowering systemic inflammation helps preserve neuronal insulin sensitivity. A Mediterranean pattern works: fish, olive oil, vegetables, nuts, and berries. Add 1 to 2g of EPA and DHA daily from fish or supplements. Minimize ultra-processed foods, refined carbs, and seed oils. Keep the polyphenols: coffee, green tea, and dark chocolate. The Mediterranean diet reduces Alzheimer's risk by roughly 30 to 40% (Scarmeas et al., 2009), and improved insulin sensitivity is a likely part of the mechanism.
Tool 5: Monitoring
Track fasting glucose under 100 mg/dL, fasting insulin under 10 µIU/mL (lower is better for the brain), HOMA-IR under 2.0, and HbA1c under 5.7%. Establish a cognitive baseline in your 40s with the MoCA and Trail Making Test, then track changes annually. If you want imaging, MRI with volumetric analysis of the hippocampus and cortical thickness, resting-state fMRI for network connectivity, and FDG-PET for brain glucose metabolism all add resolution.
How does the APOE gene change the picture?
APOE ε4 is the strongest genetic risk factor for Alzheimer's, raising risk 3 to 15 fold for people carrying two copies. APOE is a lipid transport protein, and the ε4 variant impairs lipid metabolism and worsens the effects of insulin resistance: a metabolic double hit.
If you carry ε4, metabolic interventions matter more. Ketones may be especially useful here; Henderson et al. (2009) showed cognitive improvement in ε4-positive MCI patients given ketone esters. Exercise and fasting move from optional to baseline.
Whether to test is a judgment call. Knowing your status does not change the interventions, since they are the same either way, but it may sharpen your motivation. 23andMe reports APOE status.
What does your EEG add as a dementia biomarker?
Beyond metabolism, there is a measurable electrical marker of brain aging: Individual Alpha Frequency (IAF), the peak of your alpha rhythm. For the deeper background on this band, see Decoding Alpha Waves.
The IAF trajectory with age
Young adults peak around 10 to 11 Hz. Middle age sits near 9.5 to 10 Hz. The elderly run 8 to 9 Hz. MCI and early dementia drop below 8 Hz. An IAF under 9 Hz signals high dementia risk, and it is one of the more reliable EEG predictors of cognitive decline, often more sensitive than cognitive tests. IAF reflects thalamic clock speed, how fast your brain can move information.
Why IAF slows
The basis is metabolic. Neurons running on less glucose fire more slowly. Reduced mitochondrial function lowers available energy. Thalamocortical circuits get sluggish. IAF slowing tracks the same metabolic decline described above; it is a functional readout of the energy crisis in your neurons.
IAF as early warning
IAF can be measured with QEEG in a clinical setting. A slowing IAF, especially below 9.5 Hz in your 40s or 50s, flags neuronal insulin resistance, impending cognitive decline, and a need for aggressive metabolic intervention. The signal shows up before cognitive symptoms emerge. It leads rather than lags.
Can you train IAF back up?
Neurofeedback can raise IAF. The PAF+1 protocol works at the upper edge of your alpha band. Measure your baseline IAF, say 8.5 Hz, then train from IAF to about IAF+2 Hz, in this case 8.5 to 10.5 Hz, which pulls the peak frequency upward across sessions.
Older brains need a higher dose because plasticity is reduced. Plan for 30 or more sessions, 2 to 3 times per week, 30 to 45 minutes each, clearing the roughly 300-minute total training threshold that meta-analyses associate with memory effects.
There is a paradox worth understanding. The IAF increase itself is transient and returns to baseline within about 30 days after training stops. The cognitive gains persist for 1 to 12 months, with improvements in memory, processing speed, and executive function. Training at the upper alpha edge repeatedly recruits faster thalamocortical circuits and strengthens connectivity and network efficiency. Even when the peak frequency reverts, the improved network function holds, the way strength built in the gym persists for a while after you cut back on lifting.
Combining electrical and metabolic support
Neurofeedback trains network efficiency from the top down. Ketones and fasting supply fuel from the bottom up. The two plausibly synergize, though this specific combination has not been tested head-to-head, so treat it as a reasonable extrapolation rather than a proven protocol.
If your IAF is under 9 Hz, a sequence makes sense: start the metabolic interventions, add IAF neurofeedback for 30 or more sessions, re-measure IAF every 6 to 12 months, and run quarterly booster sessions if it drifts back down. IAF training works best before advanced neurodegeneration, so the critical window of 40 to 60 is where it earns its keep.
For a comprehensive aging strategy, run both tracks. On the metabolic side: ketones, intermittent fasting, Zone 2 cardio with resistance training, and 7 to 9 hours of sleep with apnea addressed. On the electrophysiological side: IAF neurofeedback if your IAF is under 9.5 Hz, theta/beta ratio training if you have ADHD-like symptoms, and alpha asymmetry work if depression or low motivation is in the picture. For monitoring: take a QEEG baseline at 40 to 45, reassess every 3 to 5 years, and intensify everything if IAF drops under 9 Hz.
Where is the research still open?
Several questions remain unanswered. We do not yet know the optimal neuroprotective ketone level or how long it needs to be maintained. We do not know whether intermittent ketosis from 16:8 fasting matches sustained ketosis from a ketogenic diet. We cannot yet quantify neuronal insulin sensitivity directly, only brain glucose metabolism via PET. We lack preventive RCTs that start at 40 to 50 in healthy people and track for 20 or more years. And we do not know whether exercise, fasting, and the Mediterranean diet stack synergistically or hit diminishing returns when combined.
What should you do now?
If you are 44 or older, your brain is already under metabolic stress and the networks are destabilizing. If you are under 60, your neurons are still viable, stressed but salvageable. The window narrows from there. Once vascular damage accumulates and neurons die, intervention loses most of its power, and by 70 you are managing decline rather than preventing it.
The tools are accessible and mostly free. Intermittent fasting, exercise, sleep optimization, and a Mediterranean diet cost little and ask only consistency. The evidence behind them is strong. Age 44 is a biological reality, not a calendar event. Your brain tracks metabolic health, not chronological age. Pick one tool this week, 16:8 fasting five days a week is the simplest entry point, and book a QEEG baseline so you have an IAF number to watch over time.
TAGS
References
- Scarmeas (2009). Physical activity, diet, and risk of Alzheimer disease. doi:10.1001/jama.2009.1144
Related Articles
Top 7 Brain Aging Interventions After 50 (Evidence)
A neuroscientist ranks 7 brain aging interventions after 50 by evidence strength: exercise, fasting, neurofeedback, supplements, sleep, heat, and connection.
Biohacking Brain Fog: Restoring Mental Clarity
Brain fog has a measurable electrical signature. Here's the physiology, what QEEG shows, and the interventions that restore mental clarity.
Biohacking with EEG Phenotypes: Predicting Brain Function from Electrical Patterns
EEG phenotypes are stable electrical signatures that predict how you process attention, regulate mood, and respond to neurofeedback and medication.
About Dr. Andrew Hill
Dr. Andrew Hill is a neuroscientist and pioneer in the field of brain optimization. With decades of experience in neurofeedback and cognitive enhancement, he bridges cutting-edge research with practical applications for peak performance.
Get Brain Coaching from Dr. Hill →