Brain Biohacking with Photobiomodulation: Red and Near-Infrared Light Therapy
Shining light on your head to sharpen your thinking sounds like a wellness scam. The mechanism underneath it is solid biophysics, and the human data, while modest, is real.
Near-infrared light at 800 to 1100 nm passes through the skull and is absorbed by cytochrome c oxidase, which is Complex IV of the mitochondrial electron transport chain. That absorption increases ATP production, raises cerebral blood flow, and dampens neuroinflammation. The clinical translation: better memory, faster processing speed, less brain fog. Effects are small in healthy brains and larger in brains running on a compromised energy budget, which is exactly where you'd expect a mitochondrial intervention to show up most.
How Does Light Change What Your Mitochondria Do?
Your neurons are expensive to run. They burn ATP continuously to hold ion gradients, fire action potentials, and build neurotransmitters. The brain is roughly 2% of your body weight and eats around 20% of your energy.
ATP comes from mitochondria, made by the electron transport chain. A series of protein complexes passes electrons down the line and pumps protons across the inner membrane, and that proton gradient drives ATP synthase like water turning a turbine.
The choke point is Complex IV, cytochrome c oxidase. When nitric oxide binds it, or when oxidative stress and inflammation pile up, Complex IV slows down. ATP output drops. Neurons get sluggish. You feel it as brain fog, slowed thinking, and mental fatigue. If you have ever tried to think hard through a head cold or a concussion, you have felt a Complex IV traffic jam from the inside. (For a fuller breakdown of the foggy state and its circuits, see biohacking brain fog.)
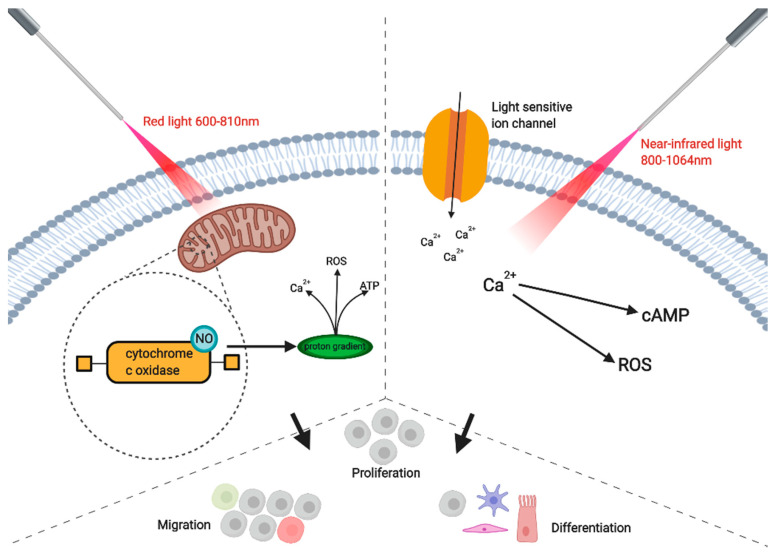
Red light, 600 to 810 nm, is absorbed directly by cytochrome c oxidase. It knocks nitric oxide off the enzyme, lifting the inhibition, and the proton gradient rebuilds. Electron transport runs cleaner and ATP rises.
Near-infrared light, 810 to 1070 nm, goes deeper into tissue, up to 30 to 40 mm. It does the same trick at Complex IV and also activates light-sensitive ion channels, raising intracellular calcium and triggering signaling cascades that add to the ATP gain.
The downstream effects follow from the energy boost. Cerebral blood flow goes up through nitric oxide release and vasodilation. Microglial activation calms, which lowers neuroinflammation. BDNF rises, which supports neuroplasticity. And as mitochondria run more efficiently, they leak fewer reactive oxygen species, so oxidative stress drops.
Which Wavelengths Actually Reach Your Cortex?
Light has to get through scalp, skull, and a few millimeters of tissue before it can do anything useful. Wavelength decides how far it gets.
Red, 630 to 660 nm, penetrates about 8 to 10 mm. It reaches scalp and the outer skull but does little for the brain itself. Good for surface tissue, weak for transcranial work.
Near-infrared, 810 to 850 nm, penetrates 30 to 40 mm and reaches the cortical surface through the skull. This is the most-studied band for transcranial PBM, and it is the band I would start with.
Deep NIR, 1070 nm, scatters and absorbs less in tissue, so in principle it reaches deeper than 810 to 850 nm. The research base is thinner than for 810 nm, so treat it as promising rather than proven.
The realistic target is cortex, the first 1 to 2 cm. Subcortical structures like the hippocampus, amygdala, and basal ganglia sit too deep for transcranial light to hit directly. They may still benefit secondhand, through better cortical blood flow and lower systemic inflammation, but that is an indirect effect.
What Does Photobiomodulation Actually Do?
Cognitive Enhancement in Healthy Adults
In healthy people the gains are real and small. Studies report faster reaction time, roughly 5 to 10% after a single session, better working memory on digit-span tasks, improved task-switching and cognitive flexibility, and less mental fatigue.
Gonzalez-Lima and Barrett (2014) found that a single 4-minute session of transcranial NIR at 1064 nm improved reaction time and sustained attention. The effect size is small to moderate. Measurable, not dramatic. If you are already sleeping well, training, and eating clean, PBM is a marginal add-on.
Traumatic Brain Injury and Concussion
A brain with a damaged energy supply has more room to gain than a healthy one.
After a concussion, microglia can stay activated for weeks to months, cerebral blood flow is often blunted, and the electron transport chain is disrupted. PBM addresses all three. It lowers neuroinflammation, restores blood flow, and helps mitochondrial function recover.
Naeser et al. (2011) found that chronic TBI patients showed improved cognition and reduced PTSD symptoms after 18 sessions of transcranial PBM using red and NIR LEDs. Case reports describe less brain fog, better sleep, and steadier mood.
Used consistently alongside neurofeedback, sleep work, and an anti-inflammatory diet, PBM can pull symptom load down. For the research on neurofeedback in TBI and concussion recovery, see the Peak Rebound research collection.
Alzheimer's Disease and Dementia
The logic tracks the mechanism: better mitochondrial function means less oxidative stress, which may mean less amyloid-beta production and accumulation, while improved cerebral blood flow delivers more oxygen and glucose and inflammation comes down.
Lim and Park (2023) reported improved cognitive function in Alzheimer's patients over a 12-week trial. Salehpour et al. (2021) reviewed the field and concluded there is potential benefit, with larger trials needed to confirm it. Status here is experimental. PBM is at most an adjunct to standard care, run with medical oversight.
Depression and Anxiety
PBM may lift mood through several routes that map onto what I see in depressed brains: increased activity in a hypoactive prefrontal cortex, more mitochondrial energy available for emotional regulation, and lower inflammatory cytokines, which are themselves linked to depression.
Several small studies show mood improvements, and in some trials the effect was comparable to antidepressants. The trials are small and the field needs larger controlled studies before strong claims hold. If anxiety is your main target, the circuit-level breakdown in biohacking anxiety pairs well with this.
How Do You Actually Run a PBM Protocol?
Devices. Helmet-style units give whole-head coverage. The Vielight combines 810 nm intranasal and transcranial LEDs; the Neuronic Neuradian 1070 uses 1070 nm for deeper penetration. Panels, like Joovv or RedTherapyCo, work well for targeted regions when positioned roughly 12 to 18 inches from the head over frontal or temporal areas.
Dose. Power density of 10 to 40 mW/cm² at the skin surface, 10 to 20 minutes per session, daily or 5 to 6 times a week, delivering about 6 to 12 J/cm² total. PBM follows a biphasic dose response, where too much light can wipe out the benefit, so stay in the window rather than overshooting it.
Timing. Morning sessions favor alertness, mood, and cognitive performance. Evening sessions favor recovery and reduced inflammation. NIR does not suppress melatonin the way blue light does, so an evening session will not wreck your sleep.
Timeline. Expect subtle changes around 2 to 4 weeks and more noticeable effects after 8 to 12 weeks of daily use. This is a slow-building intervention, not a pre-workout.
What Should You Realistically Expect?
Strong responders notice clearer thinking and less brain fog, faster mental processing, steadier mood with less anxiety, and often better sleep, especially when fog was fragmenting their nights.
Weak responders report little subjective change but may still show objective gains, such as increased cerebral perfusion on imaging.
Non-responders feel nothing. The reason is usually unclear. Their mitochondrial function may already be near optimal, leaving little headroom, or the light may not be penetrating enough to matter.
PBM moves the needle most when stacked on top of solid sleep, exercise, nutrition, and stress management. A brain that is chronically under-slept and inflamed for other reasons has bigger problems than light can solve.
Is Photobiomodulation Safe?
For most people, yes. The light is low-power and non-ionizing, so it does not damage DNA, and side effects are minimal, occasionally a mild headache in the first few sessions.
Skip it, or get medical clearance first, if any of these apply. Active cancer is a hard stop, because PBM promotes cell proliferation. Photosensitivity, from rare genetic conditions or certain medications, is a contraindication. Keep light off the thyroid, since direct exposure can stimulate it. PBM is not recommended in pregnancy, where safety data is insufficient, or in children, whose developing brains and long-term outcomes have not been studied.
For TBI and concussion recovery, depression and anxiety as an add-on to standard care, and any dementia application, run it under medical supervision rather than solo.
Bottom Line
Photobiomodulation uses near-infrared light at 810 to 1070 nm to free cytochrome c oxidase in your mitochondria, which raises ATP production and improves how the brain runs on energy.
Where the evidence sits:
- Strongest: TBI and concussion recovery, with reduced brain fog and improved cognition.
- Moderate: depression and anxiety, with mood improvements from small trials.
- Emerging: Alzheimer's and dementia, where it may slow decline.
- Modest: healthy adults, with small but measurable cognitive gains.
A starting protocol: 810 to 850 nm or 1070 nm, 10 to 20 minutes daily, with a helmet-style device like Vielight or Neuronic or a panel like Joovv, for 8 to 12 weeks before you judge it. Get sleep, exercise, and nutrition handled first, then add light if you are carrying brain fog, working through post-concussion symptoms, or chasing the last few percent of cognitive performance.
TAGS
References
- Naeser (2011). Evaluating toric implants. doi:10.1016/j.jcrs.2011.09.030
- Salehpour (2021). Betaine supplementation fails to improve body composition: a systematic review and meta-analysis. doi:10.1017/S0007114521004062
Get new articles and brain training insights by email.
No spam, unsubscribe anytime.
Related Articles
Biohacking Brain Fog: Restoring Mental Clarity
Brain fog has a measurable electrical signature. Here's the physiology, what QEEG shows, and the interventions that restore mental clarity.
Biohacking Memory: Optimizing Encoding, Consolidation, and Retrieval
A neuroscientist's guide to memory: how encoding, consolidation, and retrieval work, why most "memory problems" are attention problems, and what fixes them.
Biohacking Flow State: The Neuroscience of Peak Performance
What happens in your brain during flow, the conditions that trigger it, and the training protocols that make peak performance more accessible.
About Dr. Andrew Hill
Dr. Andrew Hill is a neuroscientist and pioneer in the field of brain optimization. With decades of experience in neurofeedback and cognitive enhancement, he bridges cutting-edge research with practical applications for peak performance.
Get Brain Coaching from Dr. Hill →