
Biohacking OCD: Targeting the Cortico-Striatal Circuit
Obsessive-compulsive disorder is a circuit problem. The cortico-striato-thalamo-cortical (CSTC) loop runs hot and over-connected, and that hyperactivity generates the intrusive thoughts you call obsessions and the repetitive behaviors you call compulsions. The checking, the counting, the washing, the rereading of an email twelve times before you send it: those are the output of a loop that cannot close.
Standard treatment is an SSRI plus exposure and response prevention. That combination helps roughly 50 to 60 percent of patients. If you are in the other 40 percent, the question becomes what else the neuroscience offers. Several targets exist beyond serotonin: glutamate modulation, methylation support, QEEG-guided neurofeedback, and behavioral training that pushes directly on the overactive circuit.
This guide walks through the neurobiology of OCD, the QEEG signatures I see in brain maps, and the interventions with evidence behind them.
Disclaimer: This is educational, not medical advice. OCD is a serious condition. Work with qualified clinicians.
What Goes Wrong in the OCD Circuit?
The CSTC loop is a feedback circuit that handles decision-making, habit formation, and behavioral control. It exists to answer one question on repeat: did that action achieve its goal? When the answer is yes, the circuit gates the signal and you move on. When the answer is no, it flags an error and you correct.
Four regions carry the load.
Orbitofrontal cortex (OFC). The OFC evaluates outcomes and assigns value to actions. In OCD it runs hyperactive and floods the loop with error signals, the felt sense that something is wrong even when nothing is.
Anterior cingulate cortex (ACC). The ACC detects conflict and monitors errors. Over-activated, it reads every error signal as a task left incomplete, a thing that must be fixed now.
Caudate nucleus (striatum). The caudate gates behavioral responses, filtering which impulses reach motor cortex. In OCD its filtering function drops. Intrusive thoughts and compulsive urges pass through that should have been screened out.
Thalamus. The relay between cortex and subcortical structures. In OCD it amplifies signals already circulating in the loop.
Put it together and you get the OCD experience at the mechanism level. The OFC fires an error signal ("did I lock the door?"). The ACC interprets that as a demand for action. The caudate fails to gate the signal, so the loop keeps firing and the urge to check returns. You check. The checking gives temporary relief, which trains the loop to repeat the whole sequence. The relief is the reinforcement. That is why willpower alone rarely closes the loop.
Which Neurotransmitters Are Dysregulated?
OCD involves at least three neurotransmitter systems, and knowing which one is the primary driver in your case changes what you target.
Serotonin
SSRIs are first-line, which tells you serotonin matters. The likely mechanism is that raising serotonin in the synaptic cleft dampens OFC hyperactivity and softens the error signaling. The response is partial. About 60 percent of patients improve. OCD involves circuit hyperactivity that serotonin partially modulates, with glutamate and dopamine carrying a significant share of the remaining load.
Glutamate
Glutamate is the brain's primary excitatory neurotransmitter, and glutamate signaling in the cortico-striatal circuit appears dysregulated in OCD. This is the most actionable target outside of prescription medication.
The supplement here is N-acetylcysteine (NAC). NAC is a glutathione precursor that also modulates glutamate by increasing reuptake, pulling excess glutamate out of the synapse and restoring homeostasis in cortico-striatal circuits. Grant et al. (2009) found NAC reduced OCD symptoms in a 12-week trial, and Oliver et al. (2015) found it effective in treatment-resistant cases. It works in both adults and children and is well tolerated.
Prescription glutamate modulators exist too. Riluzole reduces glutamate release and has shown effect in treatment-resistant OCD. Memantine, an NMDA receptor antagonist, has mixed evidence.
Dopamine
Dopamine drives motivation and reward-seeking and likely contributes to the compulsive, driven quality of the behaviors. Two clinical observations point this way: excess dopamine, such as the L-DOPA used in Parkinson's treatment, can trigger obsessive features and compulsive behavior, and some OCD patients respond to low-dose antipsychotics that block dopamine receptors. Both suggest dopamine hyperactivity in a subset of cases.
How Does Methylation Affect OCD?
The methylation cycle supports neurotransmitter synthesis (serotonin, dopamine, norepinephrine), glutathione production, and DNA repair. The folate cycle feeds it. When methylation runs poorly, neurotransmitter synthesis and antioxidant capacity both suffer.
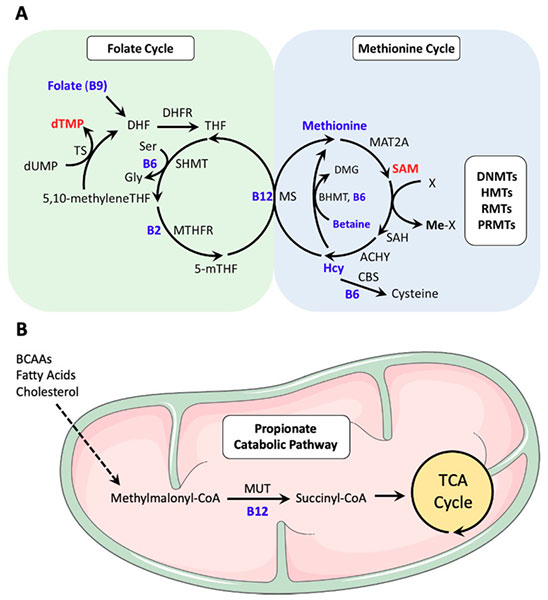
Several genetic variants slow these pathways.
MTHFR (methylenetetrahydrofolate reductase) converts folate to its active form, methylfolate. The C677T and A1298C variants reduce enzyme activity, impairing folate metabolism and downstream neurotransmitter synthesis.
COMT (catechol-O-methyltransferase) breaks down dopamine and norepinephrine. Variants set you as a fast or slow metabolizer, which shifts your baseline dopamine and norepinephrine levels.
MAO-A (monoamine oxidase A) breaks down serotonin, dopamine, and norepinephrine. Variants change the breakdown speed and alter monoamine availability.
If you carry methylation variants (test with 23andMe plus an interpretation service), the supportive nutrients are methylfolate (L-5-MTHF, 400 to 1000 mcg) rather than folic acid, methylcobalamin (B12, 1000 mcg) rather than cyanocobalamin, active B6 as P-5-P (25 to 50 mg), and NAC (1,200 to 2,400 mg) for glutathione support.
Go slow. Too many methyl donors can tip you into anxiety and agitation. Start low, increase gradually, and track your symptoms as you go.
What Does OCD Look Like on a QEEG?
When I read brain maps from clients with OCD, several electrical signatures show up repeatedly. These are clinical-observation patterns, not diagnostic markers, and they vary person to person. That variation is exactly why mapping the individual brain matters before training it. (For the full picture of what a map shows, see QEEG Brain Mapping.)
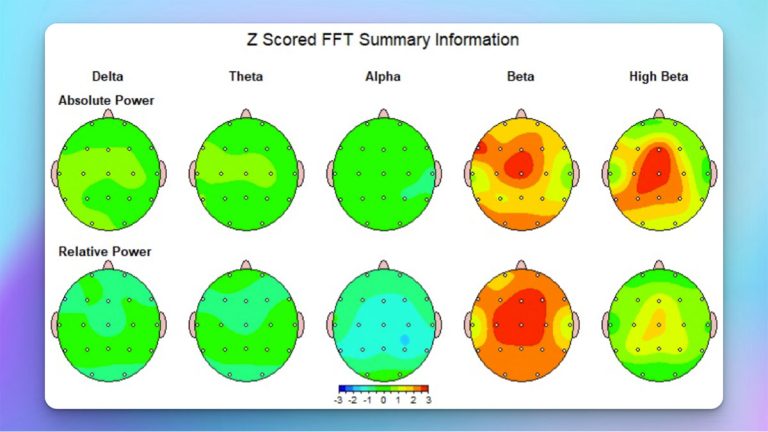
Frontal beta excess (15 to 30 Hz at Fz, F3, F4). Reflects ACC hyperactivity. Tracks with anxiety, hypervigilance, and rumination.
Frontal midline theta excess (5 to 8 Hz at Fz). Reflects ACC over-activation and the difficulty disengaging from internal focus.
Low frontal alpha (8 to 12 Hz). Indicates poor cognitive flexibility and trouble shifting attention off an obsessive thought. If you want the deeper story on what alpha does, read Decoding Alpha Waves.
Frontal alpha asymmetry (left less than right alpha). Predicts avoidance and withdrawal, and tends to show up when depression rides alongside the OCD.
Temporal lobe abnormalities. Excess theta or epileptiform activity that may feed intrusive thoughts and tics. Sometimes responds to anticonvulsants or targeted neurofeedback.
The Biohacking Interventions
1. N-Acetylcysteine for Glutamate
Start at 600 mg twice daily, total 1,200 mg. If tolerated, build to 1,200 mg twice daily, total 2,400 mg. Take it with food. Give it 8 to 12 weeks for full effect. The mechanism is glutamate homeostasis in cortico-striatal circuits plus reduced oxidative stress, and the evidence (Grant 2009, Oliver 2015) is strongest for treatment-resistant cases.
2. Neurofeedback to Retrain the Circuit
QEEG-guided neurofeedback targets the specific dysregulation your map shows, which is why I push for a map first. The protocols follow the signatures above. If you want the broader research context, start with Is Neurofeedback Legitimate?.
Frontal beta excess (anxiety, rumination): train beta (15 to 30 Hz) down at Fz, F3, F4 and train alpha (8 to 12 Hz) up for cognitive flexibility. Plan on 20 to 40 sessions.
Frontal theta excess (ACC over-activation): train theta (4 to 8 Hz) down at Fz and reward beta or SMR (12 to 15 Hz). This improves the ability to disengage attention.
Temporal lobe dysregulation: train theta and epileptiform activity down at T3, T4, T5, T6. May reduce intrusive thoughts and tics.
Alpha asymmetry (depression plus OCD): train left frontal beta up at F3 or right frontal alpha down at F4 to increase approach motivation and reduce avoidance.
Expect symptom reduction after 15 to 20 sessions, with continued gains through 40. If you cannot get to a clinic, remote neurofeedback covers many of these protocols.
3. Methylation Support When Variants Are Present
Get tested with 23andMe plus an interpretation tool such as Genetic Genie or StrateGene. With MTHFR variants, use methylfolate (400 to 1000 mcg) and methylcobalamin (1000 mcg, sublingual or injection). With COMT variants, adjust to your metabolizer status: fast metabolizers may benefit from more methyl donors, slow metabolizers should reduce methyl donors and may need magnesium. Across the board, NAC (1,200 to 2,400 mg), magnesium glycinate (300 to 400 mg), and P-5-P (25 to 50 mg) form a reasonable base. Track whether symptoms improve or worsen and adjust.
4. Meditation and Exposure-Based Practice
Mindfulness meditation strengthens prefrontal regulation of the amygdala and quiets the default mode network that drives rumination. Ten to twenty minutes a day trains two skills that bear directly on OCD: meta-awareness, noticing an obsessive thought without engaging it, and acceptance, observing an urge without acting on it. The mechanics of how that works are in Biohacking Meditation.
Pair it with exposure and response prevention (ERP), the gold-standard behavioral therapy. You expose yourself to an obsessive trigger and prevent the compulsive response. Over repeated trials the circuit learns the feared outcome does not arrive, and the obsession-to-compulsion link weakens. Meditation makes ERP more tolerable by raising your capacity to sit with discomfort and by sharpening the attention you need to notice an urge without obeying it.
5. SMR Neurofeedback for Impulse Control
SMR training (12 to 15 Hz over sensorimotor cortex) improves impulse regulation, motor inhibition, and calm focused attention, all of which work against the urge to perform a compulsion. Train SMR at C3, C4, or Cz while inhibiting theta (4 to 8 Hz) and high beta (20 to 30 Hz), across 20 to 40 sessions. The full mechanism is in SMR Neurofeedback.
What Should You Avoid?
Some interventions are unproven or risky. Lion's mane mushroom may raise BDNF, but anecdotal reports describe worsening intrusive thoughts in some people. High-dose vitamin B6 without testing can cause neuropathy above 200 mg daily. Dopamine precursors such as L-tyrosine and L-DOPA can worsen obsessive features and should not be taken without supervision.
A few things cross into dangerous. Skip research chemicals marketed as OCD cures. Do not run unsupervised neuromodulation such as tDCS or TMS without clinical guidance. And do not stop prescribed medication without medical supervision.
How Do You Sequence the Protocol?
Weeks 1 to 4, foundation. Continue or start an SSRI if prescribed, and do not stop one without medical guidance. Begin NAC at 600 mg twice daily, building to 1,200 mg twice daily after a week or two. Start ten minutes of breath-focused meditation daily. Lock in 7 to 9 hours of sleep with a consistent wake time.
Weeks 5 to 12, targeted training. Get a QEEG if you can, since it identifies the specific neurofeedback targets. Start neurofeedback on the patterns your map shows, 20 to 40 sessions over 8 to 12 weeks. Keep the NAC and meditation going. Add ERP if you are not already doing it.
Weeks 13 to 24, refine. Continue neurofeedback if symptoms persist. Extend meditation to 20 minutes daily. Add methylation testing and support if your response to everything else has been limited. Track obsession frequency and intensity and time spent on compulsions.
Month 6 and beyond, maintenance. Keep meditating to hold relapse off. Maintain NAC if it is helping. Run periodic neurofeedback booster sessions as needed.
How Do You Measure Progress?
Track the subjective markers weekly: how often intrusive thoughts arrive (daily, hourly), the intensity of the urge to perform a compulsion on a 1-to-10 scale, the minutes per day lost to compulsions, and the functional impact on work and relationships.
Pair those with objective measures. The Yale-Brown Obsessive Compulsive Scale (Y-BOCS) is the clinical standard for severity. A follow-up QEEG shows whether frontal beta, theta, and alpha asymmetry are moving toward normal. Heart rate variability tracks improving stress resilience.
Expect gradual change over 8 to 12 weeks. OCD does not resolve fast because the work is circuit retraining, and retraining a loop that has fired the same way for years takes time.
Bottom Line
OCD is hyperactivity in the cortico-striato-thalamo-cortical loop, with dysregulated serotonin, glutamate, and dopamine driving the obsessions and compulsions. Beyond SSRIs and ERP, five interventions have evidence or mechanism behind them: N-acetylcysteine at 1,200 to 2,400 mg daily to modulate glutamate, QEEG-guided neurofeedback to train down frontal beta and normalize temporal activity, meditation to strengthen prefrontal regulation and make ERP more effective, methylation support when genetic variants are present, and SMR neurofeedback to sharpen impulse control.
Response rates climb when you combine standard treatment with interventions matched to your own neurobiology. Start the NAC this week, add ten minutes of daily meditation, get a QEEG map if one is available, and work with clinicians who understand the circuit-level mechanisms.
TAGS
References
- Grant (2009). 10th Annual University of Wisconsin Land O'Lakes Bioanalytical Conference. doi:10.4155/bio.09.125
- Oliver (2015). PIPITS: an automated pipeline for analyses of fungal internal transcribed spacer sequences from the Illumina sequencing platform. doi:10.1111/2041-210X.12399
- Grant (2015). Effects of chronic alcohol consumption on neuronal function in the non-human primate BNST. doi:10.1111/adb.12289
Get new articles and brain training insights by email.
No spam, unsubscribe anytime.
Related Articles
Biohacking Brain Fog: Restoring Mental Clarity
Brain fog has a measurable electrical signature. Here's the physiology, what QEEG shows, and the interventions that restore mental clarity.
Biohacking with EEG Phenotypes: Predicting Brain Function from Electrical Patterns
EEG phenotypes are stable electrical signatures that predict how you process attention, regulate mood, and respond to neurofeedback and medication.
Biohacking Sensory and Social Processing: Optimizing Integration
How posterior sensory and frontal social networks integrate information, the QEEG signatures of dysregulation, and the interventions that improve both.
About Dr. Andrew Hill
Dr. Andrew Hill is a neuroscientist and pioneer in the field of brain optimization. With decades of experience in neurofeedback and cognitive enhancement, he bridges cutting-edge research with practical applications for peak performance.
Get Brain Coaching from Dr. Hill →