
Biohacking Memory: Optimizing Encoding, Consolidation, and Retrieval
You forget where you put your keys. A name slips away mid-conversation. You walk into a room and the reason you came in is gone. Then the worry starts: is this normal aging, early dementia, or a brain running below spec?
In most of the people who walk into my clinic with this complaint, the problem isn't memory. It's attention, sleep, or processing speed. True memory, the hippocampus-dependent formation and retrieval of episodic events, is usually intact. The bottleneck sits upstream of it.
This guide walks through what memory actually is, the three stages it moves through, and the interventions with evidence behind each one.
What Is Memory, and What Are Its Stages?

Memory is several systems running in parallel, each with its own circuit and its own failure mode.
Memory encompasses multiple systems: working memory for active manipulation, short-term memory for brief storage, and long-term memory for extended retention, including episodic (personal experiences) and semantic (factual knowledge).
The Memory Systems
Working memory is the workspace where you actively manipulate information. Capacity runs about 7±2 items (Miller's Law), duration is seconds to minutes, and it depends on the prefrontal cortex and parietal cortex. Holding a phone number in mind long enough to dial it lives here. The capacity is tight. Overload it and encoding to long-term storage fails before it starts.
Short-term memory holds information briefly without manipulating it. Capacity varies by modality (visual, verbal, spatial), duration is seconds to minutes without rehearsal, and it draws on prefrontal and temporal cortex. Remembering what someone just said long enough to respond is a short-term memory task.
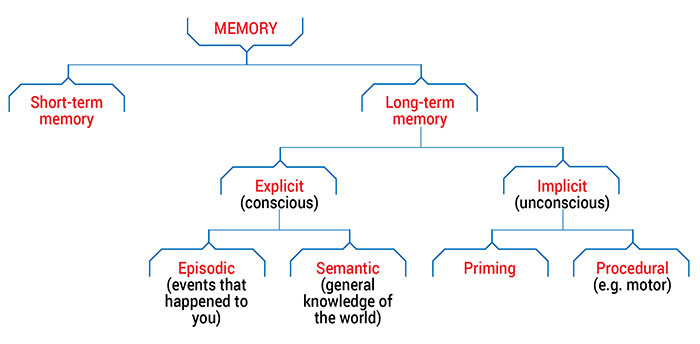
Long-term memory is stable storage that can last years to a lifetime, with essentially unlimited capacity. The hippocampus handles initial encoding; the neocortex holds the long-term version. It splits into subtypes:
- Episodic memory: personal experiences with context, time, place, and emotion. "I had dinner at that restaurant last Tuesday." This is the first to decline with aging.
- Semantic memory: facts stripped of context. "Paris is the capital of France." Vocabulary and general knowledge often hold steady or improve with age.
- Procedural memory: skills and motor sequences, riding a bike, typing. It runs on the basal ganglia and cerebellum, not the hippocampus, and it doesn't require conscious recall.
The Three Stages of Memory
Encoding converts an experience into a neural representation. It requires attention (the prefrontal cortex has to flag the information as relevant), processing speed (faster peak alpha frequency tracks with better encoding), and enough working memory to hold the material while it's processed. Encoding fails when you're distracted or multitasking, when processing speed is slow, or when working memory is already full.
Consolidation stabilizes the memory for long-term storage. It happens in two waves: initial consolidation through synaptic changes within minutes to hours (protein synthesis at active synapses), then systems consolidation, the transfer from hippocampus to neocortex during sleep, especially slow-wave sleep. Consolidation fails with insufficient deep sleep, with alcohol (which fragments sleep architecture), and with stress (elevated cortisol impairs hippocampal function).
Retrieval accesses what's stored. It needs contextual cues (memories are tied to place, emotional state, and related information), processing speed, and intact hippocampal-cortical networks. Retrieval fails when initial encoding was weak, when similar memories interfere, or when cortisol from acute stress blocks access.
Why Most "Memory Problems" Aren't Memory Problems
The complaint is usually some version of "I can't remember things anymore." The mechanism, most of the time, is an attention deficit, not a memory deficit.
If you aren't attending during encoding, because you're distracted, stressed, or running three tasks at once, the information never enters memory. It feels like forgetting. It's a failure to encode. You can't retrieve what was never written down.
Here's the test. Can you recall the information when given strong contextual cues? If yes, encoding worked and retrieval is the issue. If you still can't, even with cues, encoding likely failed in the first place.
That changes what to do. Fix attention first, then move to memory-specific strategies. Mindfulness training and the sleep and processing-speed work below all target encoding before anything else does.
How Do Sleep, Exercise, and Stress Shape Memory?
Sleep: The Consolidation Window
Consolidation happens largely while you sleep.
During slow-wave (deep) sleep, the hippocampus replays the day's newly encoded information, transfers it to the neocortex for long-term storage, and strengthens the synaptic connections formed during learning. REM sleep integrates new memories with what you already know, builds novel associations (the reason you wake with the solution to yesterday's problem), and consolidates emotional content.
Quality sleep is essential for memory consolidation, deep sleep transfers information from short-term to long-term storage, while REM sleep integrates new memories with existing knowledge.
The evidence is strong here. Sleep deprivation after learning cuts consolidation by about 40% (Walker et al., 2002). A single night of poor sleep measurably degrades next-day encoding.
The protocol:
- 7 to 9 hours total, with more than 20% deep sleep (aim for 25% if you can)
- A consistent wake time to anchor your circadian rhythm
- Stop eating 2 to 3 hours before bed, which lets blood glucose drop and supports deep sleep
- Skip antihistamine sleep aids; diphenhydramine blocks acetylcholine, the neurotransmitter memory depends on
Natural supports worth considering: melatonin at 0.3 mg (300 micrograms), not the 3 to 10 mg that overshoots the biphasic dose-response curve; magnesium glycinate or threonate at 300 to 400 mg; and L-theanine with GABA at 200 mg plus 100 to 200 mg, which work together for sleep onset. For the full picture, see biohacking sleep.
Exercise: BDNF and Neurogenesis
Exercise is one of the strongest memory interventions available, and it's free.
The mechanism: exercise raises BDNF (brain-derived neurotrophic factor) by 30 to 50% for 2 to 3 hours afterward. BDNF drives neurogenesis in the hippocampus, the formation of new neurons. It enhances synaptic plasticity, so new connections form more easily, and it improves cerebral blood flow, delivering more oxygen and glucose to the brain.
The evidence: regular exercisers carry larger hippocampal volume than sedentary peers (Erickson et al., 2011). Acute exercise before learning improves encoding. Six or more months of consistent training improves memory in older adults and slows age-related decline.
The protocol: Zone 2 cardio at a conversational pace, 30 to 45 minutes, 4 to 5 times a week; resistance training 2 to 3 times a week (it improves executive function through a different mechanism); and, when you can, exercise before a learning session to ride the BDNF window.
Stress Management: Protecting the Hippocampus
Chronic stress is corrosive to memory. Sustained cortisol shrinks hippocampal volume, measurable on MRI after months of elevated load. It impairs long-term potentiation (LTP), the cellular process underneath every memory you form. It suppresses BDNF, and it degrades both encoding and retrieval.
What helps: daily meditation (10 to 20 minutes lowers baseline cortisol and increases hippocampal gray matter), HRV training to build stress resilience, social connection to buffer the stress response, and adequate sleep, since short sleep itself drives cortisol up. If your stress sits in the body more than the mind, biohacking fight or flight covers the autonomic side.
What Are the Memory-Specific Interventions?
Nutrition: Fueling the Brain
Your brain is about 2% of body weight and burns roughly 20% of your glucose and oxygen. Nutrient gaps show up directly as worse memory.
Omega-3s (DHA/EPA): DHA is a structural component of neuronal membranes, and the brain is about 60% fat. Omega-3s support synaptic plasticity and lower neuroinflammation. Dose: 1 to 2 g per day from fish oil or algae.
B vitamins (B6, B12, folate): required for synthesizing acetylcholine, dopamine, and serotonin. Deficiency produces cognitive impairment. Most people get enough B6 and folate from diet, but B12 deficiency is common in older adults as absorption declines.
Choline: the precursor to acetylcholine, the primary memory neurotransmitter. Found in eggs, liver, and fish. Supplemental forms: Alpha-GPC at 300 to 600 mg, or CDP-choline at 250 to 500 mg.
Magnesium: required for NMDA receptor function, which LTP depends on. Most people run low. Dose: 300 to 400 mg glycinate or threonate; threonate crosses the blood-brain barrier more readily.
Creatine: raises brain ATP, your energy currency. It improves working memory and processing speed, most visibly under cognitive fatigue. Dose: 5 g per day.
Glucose: the brain's main fuel. Stable blood sugar beats sugar crashes, so build meals around complex carbs and adequate protein to avoid the spike-and-crash cycle.
Cognitive Training: Use It or Lose It
Dual n-back training loads working memory capacity. Twenty to thirty minutes daily for eight or more weeks shows gains on the task; whether those gains transfer beyond it stays contested. I'd file this as emerging, not settled.
Spaced repetition means reviewing material at widening intervals. It optimizes consolidation by forcing the effort of retrieval, which is what strengthens the trace. More detail in biohacking learning.
Learning new skills drives neuroplasticity when the activity is novel and genuinely challenging: a new language, an instrument, a complex motor skill. Pair cognitive load with social engagement, a group dance class for instance, and you get more out of the same hour.
Meditation: Attention and Hippocampal Volume
Eight weeks of daily meditation increases hippocampal gray matter density. The mechanism runs three ways: it strengthens attention control, which improves encoding; it lowers stress, which protects the hippocampus from cortisol; and it raises BDNF.
The practice is simple. Ten to twenty minutes daily, attention on the breath or body sensations. When the mind wanders, you bring it back. That return is the rep. Long-term meditators show preserved memory function with age, offsetting the normal decline.
Neurofeedback: Targeting Memory Circuits
When a QEEG brain map shows specific dysregulation, neurofeedback can train the circuit directly. The patterns I see most often in memory complaints:
Slowed peak alpha frequency (PAF). A PAF below 9 Hz tracks with slower processing speed and weaker encoding. Alpha training can nudge PAF upward, training alpha at or just above baseline over 20 to 30 sessions.
Excess frontal theta. This signals inattention and low arousal, which starves encoding. The protocol trains theta down and rewards beta or SMR at frontal sites.
Temporal lobe dysregulation. The temporal regions near the hippocampus sometimes show excess slow waves, which can reflect reduced hippocampal efficiency. The protocol trains down theta and delta at T3, T4, T5, and T6.
Timeline: 20 to 40 sessions for durable change. This is clinical observation grounded in QEEG data, not large RCTs; treat it as a targeted tool when a map points to a specific pattern.
Nootropics (Evidence-Based Only)
Caffeine plus L-theanine improves attention and working memory without the jitter. Dose: 100 mg caffeine with 200 mg L-theanine.
Bacopa Monnieri, an Ayurvedic herb, supports consolidation. Trials show improved memory in healthy adults after about 12 weeks. Dose: 300 mg of standardized extract at 50% bacosides.
Lion's Mane may raise NGF (nerve growth factor). The cognitive evidence is preliminary and needs more work. Dose: 500 to 1000 mg extract.
Ginkgo Biloba has mixed evidence; some studies show modest memory gains, others none. It may improve cerebral blood flow. Dose: 120 to 240 mg standardized extract.
Skip the racetams (limited human safety data), research chemicals (no long-term safety data), and anything sold as a "brain fog cure" without evidence behind it. If brain fog is the real issue, biohacking brain fog addresses it directly.
Age-Related Memory Decline: Normal vs. Not
Normal aging looks like this: episodic memory declines gradually, so specific events get harder to retrieve; semantic memory holds or improves, so vocabulary and general knowledge stay strong; processing speed slows (a lower PAF); and working memory capacity drops slightly.
These signs are not normal and warrant a doctor's visit: forgetting recent conversations entirely, getting lost in familiar places, personality changes, losing the ability to perform familiar tasks, and confusion about time or place.
What slows the normal decline: exercise (4 to 5 times a week, Zone 2 plus resistance), sleep (7 to 9 hours, more than 20% deep), social engagement that's both cognitive and emotional, lifelong learning that stays novel and challenging, and a Mediterranean-style diet high in omega-3s and antioxidants and low in processed food. The brain ages on its own schedule; for why the window opens earlier than most people assume, see the critical aging window.
Which Memory Techniques Actually Work?
Method of Loci (the memory palace): associate each item with a spatial location along a familiar route, then walk the route mentally to recall the sequence. It's remarkably effective for ordered lists.
Chunking: group information into meaningful units. A phone number, 5551234567, becomes 555-123-4567, three chunks instead of ten digits, which fits working memory far better.
Elaborative encoding: connect new material to what you already know. Generate examples, build a story, ask how this relates to something familiar. The links become retrieval cues.
Visual imagery: convert abstract information into vivid mental pictures. Bizarre, emotionally charged images stick best.
These techniques work, and they cost effort every time you use them. For most people, getting the foundations right, sleep, exercise, stress, returns more for less work than any mnemonic.
Your Memory Optimization Protocol
Daily:
- Morning exercise (30 to 45 minutes Zone 2) for the BDNF boost
- Meditation (10 to 20 minutes) for attention and hippocampal health
- Omega-3s, magnesium, B vitamins
- Single-task during learning, no distractions, so encoding can happen
- Sleep: 7 to 9 hours, more than 20% deep
Weekly:
- Social and cognitive engagement (group activities, novel learning)
- Review what you learned (spaced repetition)
Monthly:
- Check in: are you forgetting more than usual, and is attention the real driver?
- If memory stays a problem despite the basics, consider a QEEG and neurofeedback
Annually:
- Run a cognitive baseline (online tests for memory, processing speed, working memory)
- Track the trend: improving, stable, or declining
Bottom Line
Most "memory problems" trace back to attention, sleep, or processing speed, not to the memory system itself. The interventions that move the needle, roughly in order of leverage:
- Sleep (7 to 9 hours, more than 20% deep; consolidation lives here)
- Exercise (Zone 2 cardio 4 to 5 times a week; BDNF and neurogenesis)
- Stress management (meditation, HRV training; protects the hippocampus)
- Nutrition (omega-3s, B vitamins, magnesium, choline; fuel the brain)
- Attention training (meditation, single-tasking; improves encoding)
- Cognitive engagement (lifelong learning, social connection)
- Neurofeedback (when a QEEG reveals a specific pattern)
Mnemonic techniques and spaced repetition help, but they sit downstream of the foundations.
If you're sleeping well, exercising, managing stress, and still struggling with memory, see a doctor. Rule out the treatable causes, B12 deficiency, thyroid dysfunction, depression, medication side effects, before you write it off as aging.
The brain stays plastic, and memory systems improve at any age with the right inputs. Start with sleep tonight; everything else compounds from there.
References
- Walker (2002). Linking brain and behavior in sleep-dependent learning and memory consolidation. doi:10.1073/pnas.012689199
Get new articles and brain training insights by email.
No spam, unsubscribe anytime.
Related Articles
Biohacking Learning: Evidence-Based Strategies for Accelerated Skill Acquisition
A neuroscientist's guide to accelerated learning: spaced repetition, active recall, sleep consolidation, BDNF, and the circuits that turn practice into skill.
Biohacking Intelligence: Optimizing Cognitive Resources
You can't move IQ much, but you can train the cognitive resources that drive learning: processing speed, working memory, and implicit learning.
Biohacking Brain Fog: Restoring Mental Clarity
Brain fog has a measurable electrical signature. Here's the physiology, what QEEG shows, and the interventions that restore mental clarity.
About Dr. Andrew Hill
Dr. Andrew Hill is a neuroscientist and pioneer in the field of brain optimization. With decades of experience in neurofeedback and cognitive enhancement, he bridges cutting-edge research with practical applications for peak performance.
Get Brain Coaching from Dr. Hill →