
Biohacking Anxiety: Targeting the Circuits That Won't Shut Up
Anxiety Is a Specific Neurophysiological State
When you feel anxious, particular circuits are running hot, specific neurotransmitter systems are dysregulated, and your autonomic nervous system is parked in threat mode. The experience feels vague and overwhelming. The underlying machinery is concrete, and it leaves measurable signatures in your brain and body.
Therapy and medication help many people. If you want to understand the mechanisms and act on them directly, biohacking gives you precise levers: neurofeedback that retrains hypervigilant brain patterns, breathing protocols that shift your autonomic state in real time, and controlled stressors that build resilience at the cellular level.
Here's the neuroscience of anxiety, circuit by circuit, with evidence-based interventions matched to each target. I'll tell you what's well-established, what's clinical observation, and where we're extrapolating.
Which Brain Regions Are Overactive in Anxiety?
Anxiety recruits several regions that, when dysregulated, generate the subjective experience of threat, worry, and hypervigilance.
The Anterior Cingulate Cortex (ACC): An Error Detector in Overdrive
The ACC sits deep in the frontal cortex and runs your error-detection system. It flags mismatches between what you expected and what happened. Working normally, it helps you adjust ("That didn't work, try something else").
In anxiety, the ACC turns hypersensitive. It fires excessively and treats almost everything as a potential error. You second-guess decisions, replay small mistakes, and cannot let things go. Think of a smoke detector that goes off every time you open the oven.
EEG signature: Anxious individuals often show theta excess at frontal midline (Fz, FCz). This reflects ACC hyperactivity and tracks with rumination severity.
What you do with this: Interventions that downregulate frontal midline theta, including neurofeedback and meditation, reduce the ACC's overreactivity.
The Posterior Cingulate Cortex (PCC): The Rumination Engine
The PCC is a hub of the default mode network, the system that runs when you're not focused on an external task. It drives self-referential thinking: "What does this mean about me?"
In anxiety, the PCC becomes a rumination engine. It loops on negative self-narratives, catastrophic predictions, and old regrets. High PCC activity tracks with the inability to turn worry off.
EEG signature: Elevated alpha power at parietal sites (Pz, POz) during rest can paradoxically signal PCC hyperactivity. This is a "stuck" alpha tied to internal fixation, not the restful alpha of meditation.
Clinical note: Alpha training for anxiety often targets the PCC to break these loops and shift the brain from internal rumination toward present-moment awareness.
The Right Temporoparietal Junction (TPJ): Social Threat Detector
The right TPJ handles mentalizing, your inference of what other people intend and feel. When it runs overactive, it biases you toward reading social cues as threats. Someone glances at you and you read judgment. A friend doesn't text back and you read anger. Ambiguous social moments turn into minefields.
This shows up strongly in social anxiety. The right TPJ runs a worst-case simulation of other people's mental states. The mechanism likely involves excessive salience network activity (anterior insula, dorsal ACC), which tags neutral social stimuli as high-priority threats. This is a mechanistic extrapolation from imaging work, not a settled fact.
Fast Alpha and Poor Alpha Blocking: The Hypervigilance Signature
Alpha waves (8 to 12 Hz) normally dominate when your eyes are closed and you're at rest. Open your eyes or engage a task and alpha "blocks," dropping to free up visual and cognitive processing. You can read more on this idle-and-brake function in Decoding Alpha Waves.
In anxiety, alpha tends to be too fast (upper alpha, 11 to 12 Hz, rather than the typical 9 to 10 Hz) and poorly reactive (it doesn't block well when you engage a task).
Fast alpha reflects a brain idling hot, primed for threat and never fully at rest. Poor alpha blocking means the brain can't drop out of vigilance even when it should. Training alpha amplitude at the right frequency, and improving alpha reactivity so it blocks on cue, restores the on-off switch for vigilance.
How the Autonomic Nervous System Drives Anxiety
Anxiety lives in the body as much as the cortex. The autonomic nervous system (ANS) has two branches:
- Sympathetic: fight or flight. Accelerates heart rate, dilates pupils, releases cortisol.
- Parasympathetic (vagal): rest and digest. Slows heart rate, supports digestion and recovery.
In chronic anxiety, sympathetic tone dominates. You're physiologically stuck in low-grade threat even when you're objectively safe, and your vagal brake, the system that should calm you, is weak.
The key metric is heart rate variability (HRV), the variation in time between heartbeats. High HRV means strong vagal tone, a flexible ANS, and good stress resilience. Low HRV means weak vagal tone, a rigid ANS, and poor regulation. Anxious people typically show low HRV, a sign the parasympathetic system is failing to dampen sympathetic arousal.
Biohack #1: HRV Training to Strengthen Your Vagal Brake
HRV biofeedback is one of the most direct ways to train your ANS. You breathe at a specific rate, around 5 to 6 breaths per minute, that hits your "resonance frequency," the rhythm at which your heart rate and breathing synchronize most efficiently.
The Mechanism
When you breathe in, heart rate rises slightly (sympathetic). When you breathe out, it falls (parasympathetic). At resonance frequency (about 0.1 Hz, or 6 breaths per minute), these oscillations amplify each other and produce maximum HRV through the baroreceptor reflex.
Practicing this rhythm trains the vagus nerve to respond more strongly. Over time your baseline HRV rises, giving you more stress buffer. The vagus projects to the nucleus tractus solitarius (NTS) in the brainstem, which modulates the amygdala and prefrontal cortex. Strengthen vagal input and you enhance top-down regulation of the fear circuit.
Who Responds to HRV Training?
About 70 to 85% of people show meaningful anxiety reduction from HRV training. The remaining 15 to 30% respond poorly. Some predictors help you tell which group you're in.
Moderate-to-high baseline HRV. If your resting HF-HRV (high-frequency component) sits above 20 ms², you're likely to respond well. The people who respond best are not those with the worst HRV. A well-regulated system is trainable; a severely dysregulated one (HRV under 20 ms²) has less capacity to improve without preliminary work.
RSA trainability, the strongest predictor. RSA is respiratory sinus arrhythmia, the heart rate oscillation caused by breathing. What matters most is whether you can amplify RSA during resonance breathing. Check RSA gain across sessions 1 through 5. If RSA increases, you're likely to benefit from continued training. If it stays flat, adjust the breathing rate, tighten the guidance, or try another approach. Baseline RSA matters less than trainability. Even people with poor resting RSA improve if they can produce RSA increases during practice.
Adherence to home practice. Daily 10 to 20 minute practice between sessions is a major determinant of outcome. Clinic sessions alone aren't enough, because autonomic plasticity needs repetition. Apps like HeartMath and Elite HRV, reminders, and gamified practice all help.
Three non-responder profiles show up in the clinic. Very low HRV with poor RSA gain (HF-HRV under 15 ms², no RSA increase even with guidance): start with basic stress management through exercise and sleep, then retry HRV biofeedback, or move to neurofeedback. Heavy comorbidity (depression plus chronic pain plus trauma): multiple stressors blunt autonomic plasticity, so address comorbidities first or combine HRV with psychotherapy. Low engagement (irregular attendance, no home practice): the dose is too small for learning, so address the time and motivation barriers and use more engaging tech.
If HRV training isn't working, try neurofeedback (it targets cortical regulation directly, covered below), consider transcutaneous vagus nerve stimulation (tVNS) for direct vagal activation without training, or combine HRV with CBT and exposure therapy so the psychological and physiological approaches reinforce each other.
The Protocol
Use a device that measures HRV in real time, such as HeartMath Inner Balance, Elite HRV, or Firstbeat Bodyguard. Sit quietly and breathe at your resonance frequency (typically 5 to 6 breaths per minute; some devices calculate yours). Breathe smoothly through the diaphragm, in through the nose, out slowly through pursed lips, with the exhale longer than the inhale (try 4 seconds in, 6 seconds out). Practice 10 to 20 minutes daily.
Effects on anxiety often emerge within 2 to 4 weeks of daily practice. Multiple studies show HRV biofeedback reduces anxiety symptoms, sometimes as effectively as CBT, by retraining autonomic reactivity (Lehrer et al., 2020).
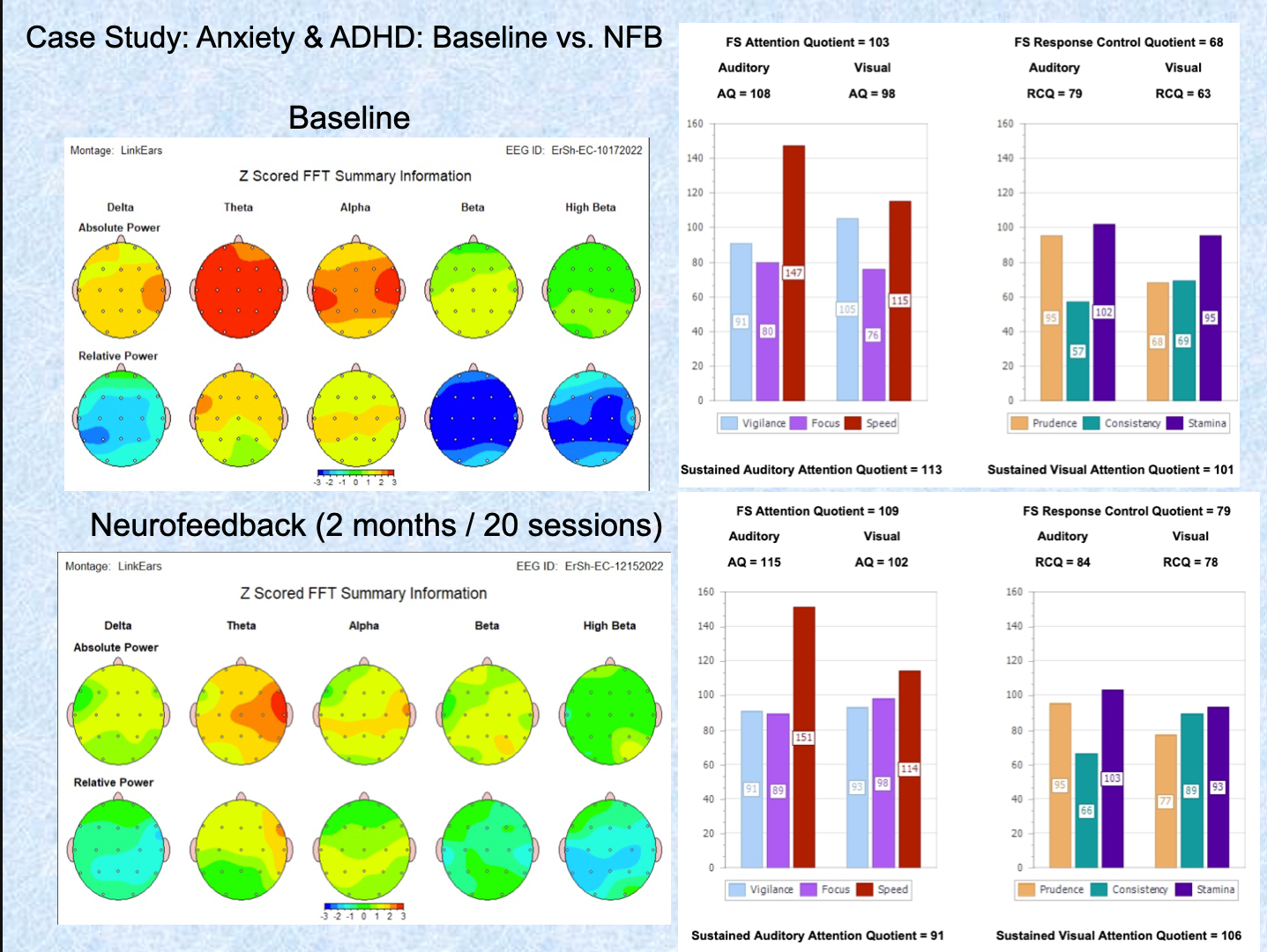
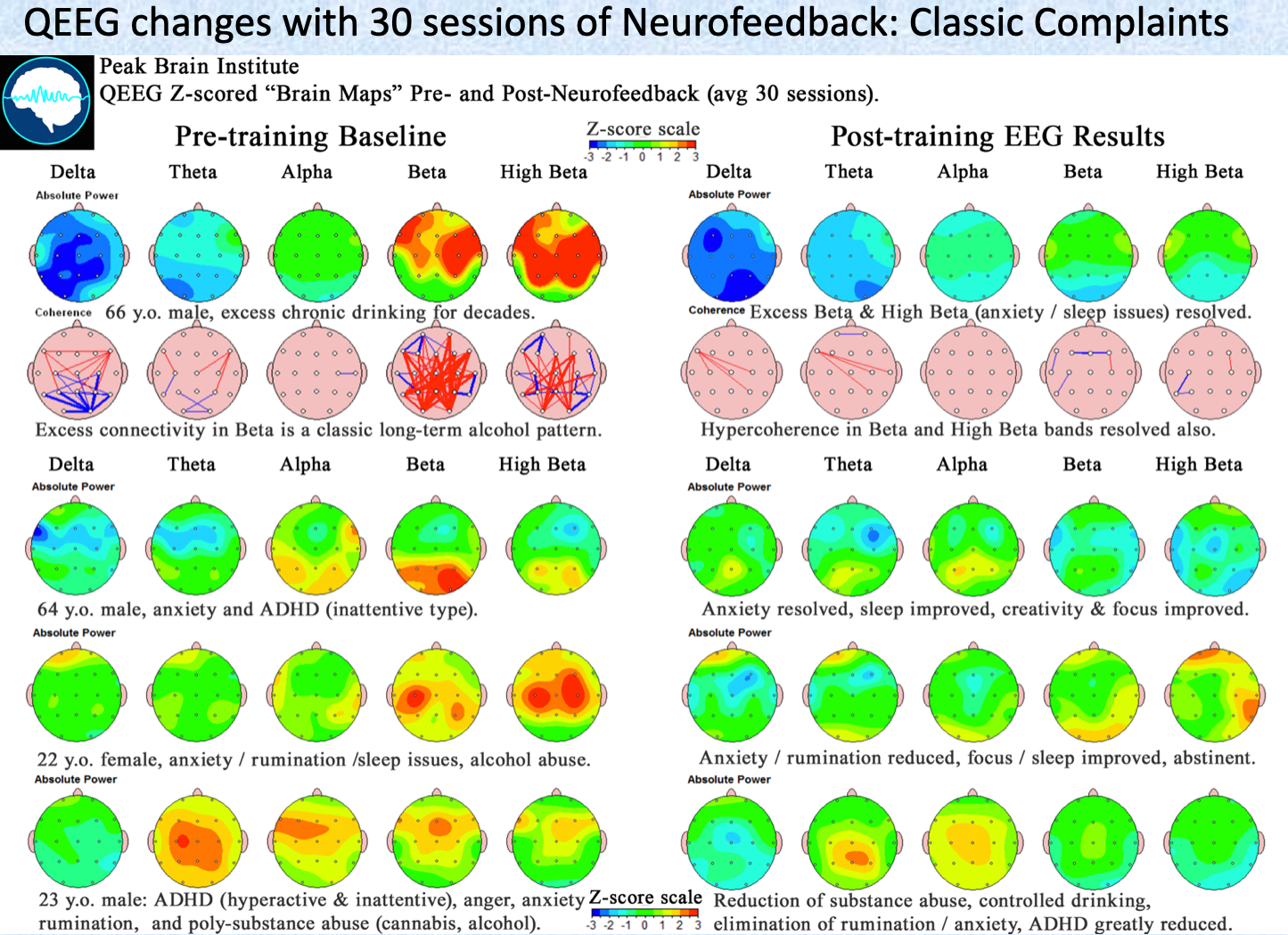
Biohack #2: Neurofeedback for Anxiety
Neurofeedback retrains specific brainwave patterns. For anxiety, the aim is to reduce hypervigilance signatures (fast rhythms, frontal theta) and strengthen calming rhythms (SMR, alpha). For the broader evidence base, see Neurofeedback for Anxiety: What the Research Shows.
Protocol 1: SMR Training (12 to 15 Hz at C3/C4)
SMR, the sensorimotor rhythm, is a narrow band of lower beta generated over the sensorimotor cortex. It marks motor stillness and calm alertness, the state you produce sitting quietly, physically relaxed but mentally aware. High SMR tracks with low muscle tension and a reduced startle response. You can go deeper on this rhythm in SMR Neurofeedback.
SMR training strengthens thalamocortical inhibition. The thalamus gates sensory input, and stronger SMR means better filtering of irrelevant stimuli, which reduces the sensory overwhelm that commonly triggers anxiety.
Train at Cz (central midline) or C3/C4 (left/right sensorimotor). Reward 12 to 15 Hz, inhibit theta (4 to 8 Hz) and high beta (20 to 30 Hz), across 20 to 30 sessions at 2 to 3 times per week. Expect reduced physical tension, fewer anxiety spikes, and improved sleep.
Protocol 2: Alpha Training (8 to 12 Hz at Pz)
The goal here is to increase alpha amplitude at posterior sites (Pz, POz) to strengthen the brain's idle state. The PCC underlying Pz is a rumination hub, and training alpha here can disrupt the default mode network's tendency to loop on negative thoughts.
Alpha oscillations reflect cortical inhibition. Training alpha at the PCC teaches the brain to stop processing self-referential worry, installing a usable off switch.
Train at Pz or POz. Reward 8 to 12 Hz (or individualize to your peak alpha frequency), inhibit theta and beta, across 15 to 25 sessions. Alpha training works best for generalized anxiety and rumination. For acute anxiety or panic, start with SMR to stabilize before adding alpha.
Protocol 3: Alpha-Theta Training (Deep Relaxation)
This protocol raises the ratio of theta (4 to 8 Hz) to alpha (8 to 12 Hz) to induce hypnagogic states, the twilight zone between waking and sleep. Eugene Peniston developed it for PTSD and addiction. It opens access to subconscious emotional material and promotes deep relaxation. For anxiety, it works once a person is stabilized, not during acute anxiety.
The hypnagogic state (high theta, moderate alpha) resembles REM sleep patterns associated with memory reconsolidation and emotional processing. It may allow anxious or traumatic memories to be re-encoded in a less threatening context. That memory-reconsolidation account is a plausible mechanism, not a closed case.
Train at Pz or Oz (parietal/occipital). Reward when theta exceeds alpha (theta/alpha ratio above 1), eyes closed, deeply relaxed, often paired with guided imagery, across 10 to 15 sessions. Do not use this for acute anxiety or panic. It's for chronic, treatment-resistant anxiety or PTSD after initial stabilization with SMR or alpha.
Which Protocol Works for Which Anxiety?
Protocols don't work equally well across anxiety types. Head-to-head data are sparse, but the pattern is clear enough to guide choices.
In direct RCT comparison for generalized anxiety, both SMR and alpha-theta reduced anxiety significantly, but SMR produced greater symptom reduction on standardized scales and more robust EEG changes tied to sensorimotor regulation. SMR is the stronger first-line choice for GAD.
Alpha-theta has the strongest evidence in trauma populations, including combat PTSD and childhood trauma, with large, durable effects on PTSD symptoms, depression, and anxiety. The mechanism matches: trauma processing benefits from the memory reconsolidation that the hypnagogic state facilitates. Reserve alpha-theta for trauma-based anxiety.
Posterior alpha has the best evidence for rumination, test anxiety, performance anxiety, and subclinical worry, by quieting the default mode network and reducing cognitive hyperactivity. It's less robust than SMR for DSM-defined anxiety disorders.
A Decision Tree for Protocol Selection
Start by identifying your anxiety profile.
Body-up anxiety (panic, hypervigilance, somatic tension, easy startle, poor sleep) points to SMR training at C3/C4/Cz, 12 to 15 Hz, across 20 to 30 sessions. Mind-up anxiety (constant worry, rumination, cognitive tension, can't turn off thoughts) points to posterior alpha at Pz/POz, 8 to 12 Hz, across 20 to 40 sessions. Trauma-based anxiety (PTSD, abuse history, flashbacks, emotional numbing) means stabilize first with SMR over 10 to 20 sessions, then move to alpha-theta over 10 to 20 sessions for trauma processing. Mixed or complex anxiety with high comorbidity calls for a QEEG first to identify the specific dysregulation, then QEEG-guided protocol selection. Read what mapping involves in the QEEG Brain Mapping guide.
If a QEEG shows excess frontal beta (15 to 30 Hz), train beta down or train SMR up to replace tense arousal with calm focus. Low posterior alpha calls for alpha-up training at Pz/O1/O2. High theta with low beta calls for SMR to raise arousal and reduce sluggishness. Frontal alpha asymmetry (left less than right) supports an alpha asymmetry protocol for withdrawal and avoidance.
What If Neurofeedback Isn't Working?
After 10 sessions with no improvement, check the protocol match first: are you training the right target for your symptoms? Verify artifact control, because EMG contamination makes training ineffective. Switch protocols (SMR if you started with alpha, or the reverse). Combine EEG with HRV biofeedback, which together raise response rates. Consider alternatives like VNS, medication, or intensive psychotherapy.
On dose: expect gradual improvement over 20 to 40 sessions. If you're seeing no change by session 15 to 20, reevaluate.
Biohack #3: Walking as Bilateral Stimulation
Walking is underrated as an anxiety intervention, and the reasons are specific.
Walking is rhythmic, alternating left-right movement, which creates bilateral stimulation, a pattern that dampens amygdala activity. The proposed mechanism: rhythmic bilateral stimulation (similar to what EMDR therapy uses) engages the cerebellar vermis, which has inhibitory connections to the amygdala, desyncing the amygdala from its fear loop and letting the prefrontal cortex reassert control. That cerebellar account is a mechanistic extrapolation.
Moderate aerobic exercise like brisk walking also stimulates endocannabinoid production, your brain's own calming chemistry. These act on CB1 receptors in the amygdala and hippocampus, reducing the fear response and enhancing extinction learning, the unlearning of fear associations. The runner's high is largely endocannabinoid, not just endorphin.
Walking in natural settings (forest bathing, or shinrin-yoku) activates the ventromedial prefrontal cortex (vmPFC), the region that inhibits the amygdala. Nature exposure reduces ACC hyperactivity, likely through lower sensory load than urban environments.
Aim for 30 to 60 minutes of walking daily, ideally in nature, at a pace brisk enough to elevate heart rate slightly while you can still hold a conversation. Add a mindfulness layer: focus on your feet hitting the ground and the rhythm of your breath, and when your mind drifts to worry, redirect to sensation. Acute anxiety drops within one session; sustained effects build over weeks.
Biohack #4: Breathing for Immediate Vagal Activation
Breath is the most direct lever you have over your autonomic nervous system. Unlike heart rate or digestion, breathing is both automatic and voluntary.
When you extend your exhale, you activate stretch receptors in the lungs. They signal the vagus nerve, which signals the NTS in the brainstem, which inhibits the sympathetic nervous system. Long exhales tell your brainstem you're safe and it can stand down.
Box Breathing (4-4-4-4)
Inhale 4 seconds, hold 4, exhale 4, hold 4, for 5 to 10 cycles. Use it for acute anxiety, panic, and pre-stress moments like meetings or presentations. The breath holds raise CO2 tolerance, which dampens the panic response. Many panic attacks are driven by hyperventilation and low CO2 (respiratory alkalosis); box breathing normalizes blood gases.
4-7-8 Breathing (Rapid Shutdown)
Inhale 4 seconds, hold 7, exhale 8, repeat 4 times. Use it for insomnia, acute anxiety, and any time you need to calm down fast. The extended hold and long exhale strongly activate the vagus nerve, and the 8-second exhale is slow enough to approach resonance frequency (about 0.1 Hz). Andrew Weil popularized this from yogic pranayama (Ujjayi breath).
Resonance Frequency Breathing (5 to 6 breaths per minute)
Inhale 5 seconds, exhale 5 (or 4 in, 6 out), for 10 to 20 minutes. Use it for daily HRV training and long-term anxiety reduction. This rate maximizes HRV by synchronizing heart rate oscillations with respiratory sinus arrhythmia, the sweet spot for vagal activation.
Biohack #5: Nootropics That Target Anxiety Biochemistry
Nootropics modulate the neurotransmitter systems involved in anxiety. They work through specific mechanisms, not through a generic "take a pill and relax."
L-Theanine (100 to 200 mg)
L-theanine raises GABA, serotonin, and dopamine, and modulates glutamate, the brain's primary excitatory neurotransmitter. Anxiety often involves excess glutamate, and L-theanine dampens that overexcitation without sedation. Green tea contains roughly 20 to 30 mg per cup; supplementation gives higher doses. The effect is relaxation without drowsiness and reduced mental chatter, and it pairs well with caffeine, cutting jitters while preserving alertness. It reduces the cortisol and heart-rate stress response during acute stress tasks (Unno et al., 2018), and meta-analyses show modest but consistent anxiolytic effects. Dose 100 to 200 mg, once or twice daily, with onset in 30 to 60 minutes.
Ashwagandha (300 to 600 mg KSM-66 extract)
Ashwagandha is an adaptogen that modulates the hypothalamic-pituitary-adrenal (HPA) axis, reducing cortisol output by normalizing glucocorticoid receptor sensitivity. Chronic anxiety keeps your stress system stuck on; ashwagandha recalibrates it, lowering baseline cortisol while preserving your acute response to real threats. Multiple RCTs show 30 to 40% reductions in cortisol and anxiety scores after 8 weeks (Chandrasekhar et al., 2012; Lopresti et al., 2019). Dose 300 to 600 mg of KSM-66 or Sensoril extract once daily, with full effects in 2 to 4 weeks. Avoid it if you have hyperthyroidism, since it can raise T4.
Magnesium Glycinate (200 to 400 mg elemental Mg)
Magnesium is a co-factor for GABA-A receptors and a natural NMDA receptor antagonist. NMDA receptors carry glutamate's excitatory signal, and blocking them lowers neural excitability, so magnesium calms overactive neurons. The glycinate form adds glycine, an inhibitory neurotransmitter that improves absorption and contributes its own calming effect; oxide and citrate forms are less bioavailable or harder on the gut. Magnesium deficiency is common and tracks with anxiety severity, and supplementation reduces anxiety in deficient individuals (Boyle et al., 2017). Dose 200 to 400 mg elemental magnesium as
References
- Boyle (2017). The Effects of Magnesium Supplementation on Subjective Anxiety and Stress-A Systematic Review. doi:10.3390/nu9050429
Get new articles and brain training insights by email.
No spam, unsubscribe anytime.
Related Articles
Biohacking Brain Fog: Restoring Mental Clarity
Brain fog has a measurable electrical signature. Here's the physiology, what QEEG shows, and the interventions that restore mental clarity.
Biohacking with EEG Phenotypes: Predicting Brain Function from Electrical Patterns
EEG phenotypes are stable electrical signatures that predict how you process attention, regulate mood, and respond to neurofeedback and medication.
Biohacking Sensory and Social Processing: Optimizing Integration
How posterior sensory and frontal social networks integrate information, the QEEG signatures of dysregulation, and the interventions that improve both.
About Dr. Andrew Hill
Dr. Andrew Hill is a neuroscientist and pioneer in the field of brain optimization. With decades of experience in neurofeedback and cognitive enhancement, he bridges cutting-edge research with practical applications for peak performance.
Get Brain Coaching from Dr. Hill →